Geographical miss during catheter-based intracoronary beta-radiation: incidence and implications in the BRIE study
Clinical study
Abstract
OBJECTIVES
We sought to determine the incidence and causes of geographical miss (GM) and to evaluate its impact on edge restenosis after intracoronary beta-radiation therapy.
BACKGROUND
Edge restenosis is a limitation of intracoronary beta-radiation therapy. Geographical miss is the situation in which the radiation source does not fully cover the injured segment and may lead to edge restenosis.
METHODS
We analyzed 175 vessels treated according to the Beta-Radiation In Europe (BRIE) study protocol. The effective irradiated segment (EIRS) and both edges were studied with quantitative coronary angiography. The edges of the EIRS that were injured constituted the GM edges. Restenosis was defined as diameter stenosis >50% at follow-up. Geographical miss was determined by simultaneous electrocardiographic-matched, side-by-side projection of the source and balloons deflated at the injury site, in identical angiographic projections surrounded by contrast.
RESULTS
Geographical miss affected 41.2% of the edges and increased edge restenosis significantly compared with non-GM edges (16.3% vs. 4.3%, respectively, p = 0.004). Restenosis was increased both in the proximal (p = 0.05) and distal (p = 0.02) GM edges compared with noninjured edges. Geographical miss associated with stent injury significantly increased edge restenosis (p = 0.006), whereas GM related to balloon injury did not significantly increase edge restenosis (p = 0.35). The restenosis in the EIRS was similar between vessels with and without GM (24.3% and 21.6%, respectively, p = 0.8).
CONCLUSIONS
Geographical miss is strongly associated with restenosis at the edges of the EIRS. This effect is more prominent when caused by stenting. Geographical miss does not increase restenosis in the EIRS.
Introduction
Intracoronary radiation therapy is a new technique for the prevention of restenosis after percutaneous coronary interventions (1–3). Catheter-based systems and radioactive stents are currently used to deliver radiation (4). The development of stenotic lesions at the edges of the segment receiving the full-prescribed dose is a potential limitation of this treatment. This phenomenon described both after radioactive stent implantation and catheter-based intracoronary radiation was termed the “edge effect” (5–7). The pathophysiology of the “edge effect” may be the result of vessel wall injury (8–10)concomitant with low-dose radiation at the edges of the irradiated segment (11,12). The term geographical miss (GM) was invented in radio-oncology to define a cause of treatment failure due to low dose radiation. In such cases, a small part of the treatment zone either escaped radiation or was inadequately irradiated because the total volume of the tumor was not appreciated and hence an insufficient margin was taken (13). This concept was translated in interventional cardiology to define those coronary segments that were injured but received low-dose radiation (14). Aims of the study were to determine the incidence and causes of GM and to evaluate the impact of this inadequate treatment on the angiographic outcome in vessels treated according to the protocol of a multicenter intracoronary beta-radiation study using a catheter-based system.
Methods
Patient selection
Patient selection
We retrospectively analyzed 149 patients treated with catheter-based beta-radiation using the Beta-Cath system (Novoste Corp., Norcross, Georgia) enrolled in the Beta-Radiation In Europe (BRIE) trial. Patients included in the radiation protocol were those with objective signs of ischemia and presence of significant de novo lesions. Out of the total population, 123 patients underwent single-vessel percutaneous transluminal coronary angioplasty and the remaining 26 patients underwent two-vessel angioplasty, giving 175 vessels in total. In 36 patients (44 vessels) GM was not interpretable, leaving 113 patients with 131 vessels for further analysis. Characteristics of patients with interpretable angiographic documentation are summarized in Table 1.
| Age (range) | 59 (35 to 85 yrs) |
| Males | 83/113 (73.4%) |
| Diabetes | 17/113 (15%) |
| Hypertension | 39/113 (34.5%) |
| Prior MI | 39/113 (34.5%) |
| Prior CABG | 5/113 (4.4%) |
| LAD | 51/131 (38.9%) |
| LCX | 28/131 (21.4%) |
| RCA | 52/131 (39.7%) |
| Balloon angioplasty | 48/131 (36.6%) |
| Rescue stenting | 12/131 (9.2%) |
| Provisional stenting | 71/131 (54.2%) |
Device description
The device consists of three components: 1) the transfer device, which stores the radiation source train and allows its positioning within the catheter; 2) the delivery catheter, which is a 5 Fr multilumen noncentered catheter that uses saline to send and return the radiation source train; and 3) the radiation source train, consisting of 12 independent cylindrical seeds that contain the radioisotope 90Sr/90Y source, encompassed by two radiopaque gold markers (30 mm in length) (4). The longitudinal distance of the “full” prescribed dose (100% isodose) coverage measured by radiochromic film is about 26 mm (15), constituting the effective irradiation length.
Dosimetry
Prescribed dose at 2 mm from the centerline of the source axis was 14 to 18 Gray (Gy), based on the reference diameter, by on-line quantitative coronary angiography (QCA), measured <3.35 mm or >3.35 mm, respectively. The radiation source remained at the treatment site for approximately 2 to 4 min to deliver the prescribed dose. Post-hoc QCA confirmed appropriate dosimetry in all treated vessels.
Definitions
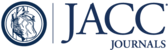
Vessel segment (VS) defined the coronary segment bordered by two side branches that encompassed the original lesion, angioplasty balloon and radiation source. The injured segment (INS) was encompassed by the most proximal and distal position of the radiopaque markers of the balloons used for dilation or stent implantation. The irradiated segment, 30-mm in length, was defined as the segment encompassed by the two gold markers of the radiation source train. The effective irradiated segment (EIRS) was the segment that received the full-prescribed dose and corresponded to the 26-mm central part of the radioactive source train. These segments are illustrated in Figure 1. The edges of the EIRS are the adjacent (proximal and distal) 5 mm coronary segments, consisting of the 2 mm inside and 3 mm outside the gold markers. These edges received low-dose radiation because of fall-off of dose in the beta-emitting 90Sr/90Y source (16,17). The highest prescribed dose was 18 Gy at 2 mm from the centerline of the source axis and the calculated dose at each millimeter away from the 100% isodose in the axial direction was expected to be 15.5 Gy at 1 mm, 11 Gy at 2 mm, 5.5 Gy at 3 mm, 2.4 Gy at 4 mm and <1 Gy at 5 mm (Fig. 1). Those edges, which were traumatized by balloon inflation (minimum inflation pressure was 6 atmospheres) or received new stent implantation during the procedure, were defined as GM edges. Noninjured edges were those that were not traumatized during the intervention.

(Left)Isodose contour rate map and radiation source train. Isodose rate contour map at a depth of 1.89 mm (10 mGy/s contour intervals) as described by National Institute of Standards and Technology. This depth (1.89 mm) illustrates an isodose model resembling the radius of the coronary artery wall. The longitudinal dose falloff may be extrapolated from this graphic. The central part of the source train (26 mm) radiates approximately full dose constituting the effective irradiation length (EIRL). (Right)A diagram of an irradiated coronary artery and the anatomical and dose-based segment definition. EIRS = effective irradiated segment; INS = injured segment; IRS = irradiated segment; IRL = irradiation length; SB = side branch; VS = vessel segment.
Determination of the GM edges
To determine whether the edges of the EIRS were injured, we retrospectively analyzed, blind to the presence or absence of restenosis and its location at follow-up, all the baseline (intervention plus radiation) angiograms. The following steps were followed: during the procedure all the interventions (balloons or stents) deflated at the site of injury and the radioactive source in place were filmed with contrast in identical angiographic projections. This approach allowed us to define the location of the various subsegments (EIRS, INS and edges) in relation to side branches and the correct matching of the angiograms in the offline analysis. A continuous electrocardiogram recording was also displayed, allowing the selection of still frames in the same part of the cardiac cycle. Multiple angiographic loops and electrocardiographic-matched still frames could be displayed simultaneously, side by side, on the screen with the Rubo DICOM Viewer (Rubo Medical Imaging, Uithoorn, Netherlands). By identifying the relationship between the EIRS and its edges relative to the INS, we determined the GM edges. Two independent cardiologists (G.S., M.C.) performed the above-mentioned analysis. There was only 10% disagreement on the presence or absence of GM and its location proximal or distal. These were borderline cases that were reanalyzed by a third reviewer (P.W.S.) with the use of transparencies before a final conclusion was determined.
In cases where one or more of the following criteria were present, the procedure was reported as noninterpretable: 1) incorrect filming of the radiation source or the balloons deflated with contrast injection; 2) more than 10° difference in the angiographic projections not allowing correct matching; and 3) interventions reported in the technician’s work sheet but not filmed.
QCA analysis
The EIRS and both edges were analyzed by QCA before and after intervention, and at six-month follow-up. All angiograms were evaluated after intracoronary administration of nitrates. The offline analysis of two orthogonal projections was performed with the CAAS II analysis system (Pie Medical BV, Maastricht, Netherlands). Calibration of the system was based on dimensions of the catheters not filled with contrast. This method of analysis has been previously validated (18–20). The following QCA parameters were computed in the VS: computer-defined minimal luminal diameter, reference diameter obtained by an interpolated method and percentage diameter stenosis. Binary restenosis was defined in every segment as diameter stenosis >50% at follow-up. This allowed the determination of restenosis in the VS (overall restenosis). Computer-defined subsegmental analysis (mean subsegment length was 5 ± 0.3 mm, depending on the length of the analyzed VS) was also performed. In each subsegment, percentage diameter stenosis was also automatically calculated. This allowed the determination of restenosis in relation to the dose-based subsegments, which was termed regional restenosis.
Determination of the restenosis location
Three observers analyzed all the films that appeared to have restenosis at the follow-up angiogram. The printouts of the pre-, post- and follow-up angiograms, in two orthogonal projections, with the subsegmental analysis and the dose-based subsegments superimposed, were compared. The observers designated the location of the computer-defined QCA subsegments with restenosis in relation to the dose-based segments. Restenosis was classified as restenosis in the EIRS, edge restenosis (proximal or distal) and restenosis outside the irradiated segment. It is important to realize that the criterion for binary restenosis might be fulfilled in more than one subsegment in the same VS.
Statistical analysis
Continuous data are presented as mean values; discontinuous data are presented as percentages. Differences in restenosis rates between edges with and without GM were evaluated with chi-square or Fisher exact tests as appropriate. Because the behavior of different segments in the same vessel and the behavior of different vessels in the same patient may not be independent, the relation between GM and edge restenosis was further analyzed by logistic regression analysis, using generalized estimation equation modeling techniques to correct for possible within-patient effects. The presented odds ratios (OR) and 95% confidence intervals (CI) are based on these analyses. Statistical significance of all tests was defined at the p < 0.05 level.
Results
Incidence and causes of GM
Vessels
Incidence and causes of GM
Vessels
A total of 131 vessels were interpretable. The incidence of GM was 67.9% (Table 2).
| Noninterpretable vessels | 25.1% (44/175) |
| Interpretable vessels | 74.9% (131/175) |
| Noninjured vessels | 32.1% (42/131) |
| GM vessels | 67.9% (89/131) |
| Vessels with GM proximal only | 37% (33/89) |
| Vessels with GM distal only | 41.5% (37/89) |
| Vessels with GM both proximal and distal | 21.5% (19/89) |
Edges
In each vessel, both proximal and distal edges of the EIRS were analyzed, giving in total 262 edges. Out of the 89 vessels with GM, 70 had one GM edge, proximal or distal, and in 19 vessels both edges were injured, giving in total 108 GM edges. The incidence of GM at the edges was 41.2%. The location proximal and distal was comparable (Table 3).
| Noninterpretable edges | 25.1% (88/350) |
| Interpretable edges | 74.9% (262/350) |
| Noninjured edges | 58.8% (154/262) |
| GM edges | 41.2% (108/262) |
| Proximal GM edges | 48.2% (52/108) |
| Distal GM edges | 51.8% (56/108) |
Procedural causes of GM
The following reasons were responsible for the GM: 1) development of procedural complications (additional stent implantation postradiation) that extended the treatment beyond the margins of the EIRS (52.8%, 57/108) (unexpected GM); 2) the INS from prior inflations was not appropriately covered by the source (34.2%, 37/108), termed as lack of accurate matching; and 3) treatment of long lesions requiring balloons or stents longer than 26 mm (EIRS) and lack of availability of longer (>30 mm) radiation source (13%, 14/108).
Restenosis rate
Follow-up angiograms were available in 115 out of 131 vessels. The restenosis rate in the EIRS was 23.5%. The presence or absence of GM did not affect the incidence of restenosis in the EIRS (24.3% and 21.6% respectively, p = 0.8). The restenosis in the proximal edge was 9.5% and in the distal edge 8.7%. Because binary restenosis can be encountered more than once per VS (either in the EIRS or at the edges) the summation of the regional restenosis rate is higher than the restenosis rate in the VS. There were three vessels with restenosis in both the EIRS and the proximal edge and four vessels with restenosis in both EIRS and the distal edge. There were no cases with restenosis in both edges.
Generalized estimation equation analysis, which was used to account for within-patient effects, showed that the probability for restenosis at the edges of the EIRS depended on the GM (p = 0.0039), but not on distal/proximal lesion location (p = 0.6) or the device (balloon/stent) used (p = 0.1).
Regional restenosis rate in relation to GM
In each of the 115 vessels (101 patients), the impact of GM on restenosis was analyzed in both proximal and distal edge (230 edges). Geographical miss significantly increased the incidence of restenosis at the edges of the EIRS compared with lesions without GM (4.35% vs. 16.3%, p = 0.004). This effect was observed both in the proximal (5.56% vs. 16.28%, p = 0.05) and distal (3.03% vs. 16.33%, p = 0.02) edges and seems to be more pronounced at the distal edge (OR = 5.3) compared with the proximal (OR = 3.2). The OR and the CI are presented in Figure 2.

Difference in the restenosis rate in the proximal distal and both edges of the effective irradiated segment between geographical miss (GM) and noninjured edges. White bars= no GM; black bars= GM. CI = confidence interval; OR = odds ratio.
Impact of GM on the restenosis rate in relation to the type of injury
Out of the 230 interpretable edges, 84 (36.5%) were related with balloon angioplasty termed as balloon edges (BE) and 146 (63.5%) with stent implantation termed as stent edges (SE). The incidence of GM at the BE and the SE was comparable (33.4% and 43.8%, respectively). At the SE, GM increased the incidence of restenosis significantly compared with edges without GM (3.66% vs. 18.75%, p = 0.006). At the BE, GM did not significantly increase the incidence of restenosis (5.36% vs. 10.71%, p = 0.35). The OR and the CI are presented in Figure 3.

Difference in edge restenosis between geographical miss (GM) edges associated with stent and balloon injury and noninjured edges. White bars= no GM; black bars= GM. CI = confidence interval; OR = odds ratio.
Discussion
This study reports on the incidence and causes of GM and its implications on edge restenosis in vessels treated with intracoronary beta-radiation according to the BRIE protocol. By careful retrospective angiographic analysis of all vessels treated with the same radiation system, we defined the effect of the injury on those areas located at the margins of the source where the delivered dose was potentially rather low.
Dosimetric zones
In any given vessel undergoing an intervention followed by radiotherapy there are six possible combinations of injury and irradiation: 1) segments injured and fully irradiated (received the prescribed dose), representing the ideal treatment; 2) segments injured and receiving less than the prescribed dose defined as GM segments; 3) segments injured and receiving no dose (falling into the category of conventional interventions); 4) segments noninjured and receiving a full dose; 5) segments noninjured and receiving a low dose, which represents a well-applied treatment because there is no indication of any adverse impact from low-dose radiation without injury after either beta (15)or gamma radiation (21); and 6) segments noninjured and receiving no radiation, falling into the category of natural progression of atherosclerosis.
Geographical miss occurred in 67.9% of the vessels and 41.2% of edges analyzed. This concept requires the concurrence of two conditions: low-dose radiation and injury. It is a dose-related term rather than an anatomical one. Injury outside the field of radiation or low-dose irradiation of noninjured tissue cannot be termed GM.
Stimulatory effect of low-dose radiation
The stimulatory effect of low-dose radiation on smooth muscle cell proliferation has been previously reported in a swine coronary balloon overstretch injury model (11). In the low-dose radiation group (10 Gy), neointima was composed of smooth muscle cells with a marked increase in inflammatory cells and less medial and intimal fibrosis as compared with higher dose groups (15 and 20 Gy) and the control group. Similarly, after low-activity radioactive stent implantation (1.0 μCi) in a porcine model, neointimal hyperplasia was significantly greater than that after nonradioactive stenting (12). Our group reported a late loss in injured edges treated with the same system that was higher than that demonstrated in the noninjured edges (14)and in previous studies after balloon angioplasty or stent implantation (22,23). In a three-dimensional volumetric intravascular ultrasound (IVUS) investigation, our group again observed a decrease in lumen volume at the edges because of an increase in plaque volume not accommodated by vessel enlargement (7). In patients receiving 6 to 12 μCi 32P radioactive stents, where GM systematically occurs because of the current balloon technology (6), 50% edge restenosis was reported compared with 0% in-stent (5).
Proximal versus distal
Geographical miss increased restenosis in both edges of the EIRS. This effect seems to be more prominent at the distal edge compared with the proximal. The smaller lumen distally attributable to normal tapering of the vessels and the even less effectively irradiated proximal edge because of its larger diameter may also be the cause. Comparing the values of restenosis proximal and distal at the GM edges, we can see that they are identical in the range of 16.3%. What makes the OR higher for the distal edge is the increased incidence of restenosis in the noninjured proximal edges. Our group has reported this through analysis of the noninjured edges of irradiated segments by three-dimensional IVUS. Greater increase in the plaque volume in the proximal edges compared with the distal (27% vs. 9.2%, respectively) was reported (15). Nonmeasurable vessel injuries (guiding catheter guidewires) were hypothesized as the cause. Rheological factors may play an important role and careful shear stress analysis could elucidate the cause of restenosis at the proximal edge (24).
Balloon versus stent injury in relation to GM
Geographical miss related to stent injury is more prominently associated with edge restenosis than is GM related to balloon injury. The mechanisms involved in restenosis after balloon angioplasty are different compared with these of stenting. Negative remodeling and elastic recoil are the causes of restenosis after balloon angioplasty, as opposed to neointimal formation after stent implantation (25). Absence of negative remodeling has been reported at the edges of the irradiated segments after balloon angioplasty (14). This might partly compensate for the stimulatory effect of radiation on plaque growth at the balloon-injured GM edges, making the combination less harmful.
The acute injury after stenting differs from that of the coronary balloon angioplasty (8). The stent is a foreign body and produces a permanent strain on the vessel wall, resulting in a chronic injury and a prolonged stimulus for neointimal formation (26). It is logical to conclude that the greater and more prolonged the injury, the greater the impact on plaque growth, and subsequently on restenosis, in conjunction with low-dose radiation. In our study, significantly higher late loss was observed in the irradiated segment in patients treated with balloons compared with the stent-treated patients (0.14 mm vs. 0.44 mm respectively, p = 0.001).
This observation is in keeping with the other serious adverse effects of the combination of stenting and radiation, such as delayed stent thrombosis (27)and late stent malapposition (28).
Study limitations
This study is not placebo-controlled and the effect of a sham source on injured coronary segments has not been evaluated.
Only one type of radiation delivery catheter using the beta-source 90Sr/90Y has been evaluated. Thus, the effect of other systems using centering balloons and different sources or gamma-radiotherapy on the GM edges cannot be extrapolated from our results.
Balloon inflation or stent implantation was considered the only source of injury. Minor injuries from guiding catheters, guidewires or radiation delivery catheters cannot be completely ruled out.
Only binary restenosis data are quoted and the determination of GM is qualitative because there was no QCA methodology available at the time to measure the length of the GM.
Conclusions
Geographical miss is strongly correlated with the development of restenosis at the edges of the EIRS. This is a local phenomenon with a specific pathophysiology (combination of injury and low-dose radiation) and is different from the restenosis observed in the EIRS. This effect was observed in both edges of the EIRS and seems to be more pronounced at the distal edge compared with the proximal. Geographical miss related to stent injury is associated with higher edge restenosis compared with GM related to balloon injury. Geographical miss did not increase the incidence of restenosis in the EIRS. If GM can be eliminated, the results of intracoronary beta-radiation will be improved.
1. : "Catheter-based radiotherapy to inhibit restenosis after coronary stenting". N Engl J Med 1997; 336: 1697.
2. : "Endovascular beta-radiation to reduce restenosis after coronary balloon angioplasty: results of the Beta Energy Restenosis Trial (BERT)". Circulation 1998; 97: 2025.
3. : "Inhibition of restenosis with beta-emitting radiotherapy: report of the Proliferation Reduction with Vascular Energy Trial (PREVENT)". Circulation 2000; 102: 951.
4. : Handbook of Vascular Brachytherapy . London: Martin Dunitz Ltd1998: 41.
5. : "Short- and intermediate-term results of (32)P radioactive beta-emitting stent implantation in patients with coronary artery disease: the Milan Dose-Response Study". Circulation 2000; 101: 18.
6. : "I like the candy, I hate the wrapper: the (32)P radioactive stent". Circulation 2000; 101: 3.
7. : "Geometric vascular remodeling after balloon angioplasty and beta-radiation therapy: a three-dimensional intravascular ultrasound study". Circulation 1999; 100: 1182.
8. : "Restenosis and the proportional neointimal response to coronary artery injury: results in a porcine model". J Am Coll Cardiol 1992; 19: 267.
9. : "Balloon angioplasty. Natural history of the pathophysiological response to injury in a pig model". Circ Res 1985; 57: 105.
10. : "Restenosis after experimental angioplasty. Intimal, medial, and adventitial changes associated with constrictive remodeling". Circ Res 1995; 76: 996.
11. : "Intracoronary irradiation: dose response for the prevention of restenosis in swine". Int J Radiat Oncol Biol Phys 1996; 36: 767.
12. : "Effects of endovascular radiation from a beta-particle-emitting stent in a porcine coronary restenosis model. A dose-response study". Circulation 1996; 94: 2364.
13. : The Treatment of Malignant Disease by Radiotherapy . London: Edward Arnold Ltd1963.
14. : "Geographic miss: a cause of treatment failure in radio-oncology applied to intracoronary radiation therapy". Circulation 2000; 101: 2467.
15. : "Three-dimensional intravascular ultrasound assessment of non-injured edges of β-irradiated coronary segments: a clue to understanding the “edge effect.”". Circulation 2000; 102: 1484.
16. : "Calibration and characterization of beta-particle sources for intravascular brachytherapy". Med Phys 1998; 25: 339.
17. : "Dosimetric considerations for catheter-based beta and gamma emitters in the therapy of neointimal hyperplasia in human coronary arteries". Int J Radiat Oncol Biol Phys 1996; 36: 913.
18. : "Experimental validation of geometric and densitometric coronary measurements on the new generation Cardiovascular Angiography Analysis System (CAAS II)". Cathet Cardiovasc Diagn 1993; 30: 104.
19. : "Calibration using angiographic catheters as scaling devices: importance of filming the catheters not filled with contrast medium". Am J Cardiol 1992; 69: 1377.
20. : Quantitative Coronary Angiography in Clinical Practice . Dordrecht/Boston/London: Kluwer Academic Publishers1994.
21. : "Safety of intracoronary gamma-radiation on uninjured reference segments during the first 6 months after treatment of in-stent restenosis: a serial intravascular ultrasound study". Circulation 2000; 101: 2227.
22. : "A comparison of balloon-expandable-stent implantation with balloon angioplasty in patients with coronary artery disease. Benestent Study Group". N Engl J Med 1994; 331: 489.
23. : "A randomized comparison of coronary-stent placement and balloon angioplasty in the treatment of coronary artery disease. Stent Restenosis Study Investigators". N Engl J Med 1994; 331: 496.
24. : "Coronary stent implantation changes 3-D vessel geometry and 3-D shear stress distribution". J Biomech 2000; 33: 1287.
25. : "Arterial remodeling after coronary angioplasty: a serial intravascular ultrasound study". Circulation 1996; 94: 35.
26. : "Prolonged proliferative response of smooth muscle cells after experimental intravascular stenting". Eur Heart J 1995; 16: 785.
27. : "Late coronary occlusion after intracoronary brachytherapy". Circulation 1999; 100: 789.
28. : "Late stent malapposition occurring after intracoronary beta-irradiation detected by intravascular ultrasound". J Invasive Cardiol 1999; 11: 651.
Abbreviations
| BE | balloon edges |
| BRIE | Beta-Radiation In Europe study |
| CI | confidence interval |
| EIRS | effective irradiated segment |
| GM | geographical miss |
| Gy | Gray |
| INS | injured segment |
| IVUS | intravascular ultrasound |
| OR | odds ratio |
| QCA | quantitative coronary angiography |
| SE | stent edges |
| VS | vessel segment |
{kind=link}
{kind=link}
{kind=link}