Left atrial volume as an index ofleft atrial size: a population-based study
Clinical study: left atrial size
Abstract
Objectives:
We studied left atrial volume (LAV) as an index of atrial size.
Background:
Increased left atrial dimension (LAD) measured by M-mode echocardiography is a risk factor for atrial fibrillation, stroke, and death.
Methods:
A random sample of residents of Olmsted County, Minnesota, age ≥45 years (n = 2,042) underwent Doppler echocardiography with assessment of LAD and LAV. A subgroup of the population (n = 767) with no cardiovascular disease and normal systolic and diastolic function was used to develop reference ranges for LAD and LAV. In the total population, the prevalence of left atrial enlargement and the association between cardiovascular disease and left atrial size as determined by both indexes were assessed.
Results:
In the normal subgroup, both indexes were associated with gender and body size, thus models controlling for body size were used to determine gender-specific reference ranges for LAD and LAV. In the total population, left atrial enlargement was common, with a prevalence of 18% (men) and 12% (women) using LAD/body surface area (BSA) and of 16% (men and women) using LAV/BSA. The agreement between the indexes was only fair (kappa = 0.53). Adjusting for age and gender, LAV/BSA was more strongly associated with the presence of cardiovascular diseases than LAD/BSA.
Conclusions:
We described a simple technique of measuring LAV, examined methods for indexing LAV, and described its normal range in a large, healthy reference cohort. Further, we find that in the community, left atrial enlargement is common and reflects the burden of cardiovascular disease.
Introduction
As measured by M-mode echocardiography, an increase in left atrial dimension (LAD) is associated with cardiovascular disease and is a risk factor for atrial fibrillation, stroke, and death (1,2). It has been suggested that left atrial volume (LAV) may be a superior index of left atrial size (3). Methods to calculate LAV (4,5)have been described, but no standardized method has been widely adopted. Few studies have compared LAD and LAV. Further, the distribution of LAV in subjects without cardiovascular disease has not been well described. Moreover, there is little agreement on how to account for body size, age, or gender in setting the most appropriate normal values for LAV. These factors have hindered widespread reporting of LAV.
We used a simple and feasible method to assess LAV in 2,042 randomly selected residents of Olmsted County, Minnesota, older than age 45 years. Our objectives were to examine the influence of age, gender, and body size on LAD and LAV in a reference subset of the population without cardiovascular disease or cardiac dysfunction and to provide adjusted reference ranges of LAD and LAV. Second, we evaluated the strength of the association between LAD and LAV and the presence of cardiovascular disease to determine if either index better reflected the effect of cardiovascular disease on left atrial remodeling. Finally, we defined the prevalence of left atrial enlargement in the population, as assessed by each index, and examined the agreement between LAV and LAD in defining left atrial enlargement.
Methods
This study was approved by the Mayo Foundation Institutional Review Board, and subjects gave written informed consent.
Study setting
The characteristics of the Olmsted County, Minnesota, population and its unique resources for population-based epidemiologic research have been described (6,7).
Population sampling, subject recruitment, and enrollment
Randomly selected residents of Olmsted County age ≥45 years were invited to participate. A sampling fraction of 7% was applied within each of the gender- and age- (five years) specific strata. Subjects within each wave of invitations were screened and recruited before initiating subsequent waves in the three years ending in September 2000. Of the 4,203 subjects invited, 2,042 (49%) participated. Analysis of the medical records of the first 1,000 invited subjects revealed no clinically significant differences between participants and nonparticipants.
Medical record review
Epidemiologic research in Olmsted County is feasible because all care providers have a unified medical record indexed and maintained by the Rochester Epidemiology Project. Each subject’s medical record was reviewed by trained nurse abstractors using established criteria for hypertension (8), myocardial infarction (9), and congestive heart failure (10). In addition, clinical diagnoses of coronary artery disease and atrial arrhythmias were recorded.
Doppler and two-dimensional (2D) echocardiography
All echocardiograms were performed by one of three registered diagnostic cardiac sonographers with the same echocardiographic instrument (HP-2500) according to a standardized protocol and interpreted by one echocardiologist (M. M. R.). Two-dimensional and color Doppler imaging were performed to screen for valvular stenosis or regurgitation.
Assessment of cardiac structure
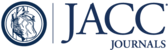
The LAD was measured by 2D-guided M-mode echocardiography obtained in the parasternal short-axis view at the base of the heart according to American Society of Echocardiography recommendations (11). Three LADs were used to calculate LAV as an ellipse using the formula: LAV = π/6 (SA1· SA2· LA) , where SA1= the M-mode LAD and SA2and LA are measurements of short- and long-axis in the apical four-chamber view (Fig. 1) (12)at ventricular end-systole. Body size variables used for indexing included body surface area (BSA) (m2), body mass index (BMI) (kg/m2), and height (cm).

(Left)Parasternal short-axis M-mode left atrial dimension. (Right)Apical four-chamber view demonstrates short and long axes.
Assessment of ejection fraction (EF)
In each subject, measurement of EF by M-mode (modified Quinones formula), quantitative 2D (biplane Simpson method of disks), and semiquantitative 2D (visual estimate) methods was performed as previously described (13,14).
Assessment of diastolic function
Pulsed-wave Doppler examination of mitral (before and with Valsalva maneuver) and pulmonary venous inflow and Doppler tissue imaging of the mitral annulus were performed in each subject. Diastolic function was categorized as: normal, impaired relaxation (grade I), pseudonormalized filling (grade II), and restrictive filling (grade III to IV), as previously described and validated (15,16).
Reference subgroup
Of the 2,042 participants, 1,020 had no history of cardiovascular, renal, or pulmonary disease and were taking no cardiovascular medications. Of these, 767 subjects had normal EF (>50%), no wall motion abnormalities, normal diastolic function, no valve disease, and normal sinus rhythm. These 767 subjects form the normal subgroup.
Statistical methods
Continuous variables are summarized as the mean ± 1 SD, and comparisons between subjects included or excluded from the reference group used the Wilcoxon rank-sum test. Categorical variables are summarized as a percentage of the group total, and the chi-squared test was used for comparisons between subjects included in the reference groups and those subjects who were excluded. For the reference subgroup, the Spearman correlation coefficient was used to assess the bivariate or pair-wise association of left atrial size parameters with age and body size. In addition, linear regression models were used to assess the joint association of age, gender, and body size with left atrial size. The prevalence of left atrial enlargement was estimated in the total population by using the empirical 95th percentile for LAD/BSA and LAV/BSA from the reference subgroup, and the association of prevalent cardiovascular abnormalities with prevalent left atrial enlargement was summarized by using the odds ratio with corresponding 95% confidence intervals (CIs). To compare the strength of association of LAD/BSA and LAV/BSA with cardiovascular abnormalities, the area under the receiver operating characteristic curve for each index of left atrial size was estimated and compared by the methods of DeLong et al. (17). Comparisons between the area under the curve for LAV/BSA and LAD/BSA were done unadjusted and adjusted for age and gender.
Results
Measurement of LAD was possible in 1,975 of the total population-based cohort of 2,042 subjects (97%) and in 750 of the 767 subjects (98%) in the reference subgroup. Measurement of LAV was possible in 1,888 of the 2,042 subjects (92%) and in 727 of the 767 subjects (95%) in the reference subgroup. Data to calculate BSA were missing in two of the subjects with LAV measurement.
LAD and LAV in normal subjects
Clinical characteristics of subjects in the total population and stratified by inclusion or exclusion from the reference subgroup are summarized in Table 1. The reference subgroup contained 300 obese participants (BMI >28 kg/m2). The LAV/BSA for obese participants (mean ± SD, 22.85 ± 5.40 ml/m2) was slightly larger than for lean participants (BMI ≤ 28 kg/m2) who had a mean LAV/BSA of 21.46 ± 5.14 ml/m2.
| Variables | Total Population(n = 2,041) | Reference Subgroup(n = 767) | Abnormal Subgroup*(n = 1,274) | p Value | |||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | ||
| Women, % | 51.84 | NA | 53.72 | NA | 50.71 | NA | 0.1876 |
| Age, yrs | 62.73 | 10.54 | 56.72 | 7.75 | 66.35 | 10.35 | < 0.0001 |
| BSA, m2 | 1.90 | 0.23 | 1.89 | 0.23 | 1.90 | 0.24 | 0.2974 |
| BMI, kg/m2 | 28.44 | 5.31 | 27.62 | 4.73 | 28.94 | 5.57 | < 0.0001 |
| Height, cm | 168.12 | 9.96 | 168.99 | 9.66 | 167.60 | 10.10 | 0.0021 |
| LAD, cm | 3.91 | 0.63 | 3.68 | 0.51 | 4.05 | 0.66 | < 0.0001 |
| LAV, ml | 47.35 | 17.38 | 41.86 | 11.91 | 50.79 | 19.29 | < 0.0001 |
Bivariable analysis showed that LAD and LAV were larger in men and increased with body size or relative weight (Table 2). There was a weak association of age with LAV.
| Variables | LA Dimension | LA Volume | ||
|---|---|---|---|---|
| Spearman (R2) | p Value | Spearman (R2) | p Value | |
| BSA | 0.463 | < 0.0001 | 0.542 | < 0.0001 |
| BMI | 0.448 | < 0.0001 | 0.411 | < 0.0001 |
| Height | 0.299 | < 0.0001 | 0.429 | < 0.0001 |
| Age | 0.0003 | 0.9919 | −0.086 | 0.0208 |
| Female gender | −0.357 | < 0.0001 | −0.408 | < 0.0001 |
Linear regression models incorporating gender, age, and body size indexes (Table 3) accounted for 12% to 26% of the variability in LAD in the reference subgroup, with higher R2values for models incorporating BSA and BMI than those incorporating height. In particular, addition of BSA to the model with age and gender increased the R2from 12% to 23% and removed the effect of gender. When BMI was added to age and gender, the R2increased from 12% to 26%, without changing the association with gender. Height had little additional impact on LAD, given age and gender, with R2remaining at 12%.
| Variables | LA Dimension | LA Volume | ||||
|---|---|---|---|---|---|---|
| Parameter Estimate* | Confidence Intervals | p Value | Parameter Estimate* | Confidence Intervals | p Value | |
| Age | 0.034 | 0.00, 0.07 | 0.0344 | −0.29 | −1.10, 0.52 | 0.4785 |
| Female gender | −0.35 | −0.42, −0.29 | < 0.0001 | −9.58 | −11.19, −7.97 | < 0.0001 |
| Model summary | R2= 0.1193 | < 0.0001 | R2= 0.1646 | < 0.0001 | ||
| Age | 0.07 | 0.04, 0.10 | < 0.0001 | 0.54 | −0.22, 1.30 | 0.1609 |
| Female gender | −0.05 | −0.14, 0.03 | 0.2289 | −1.77 | −3.77, 0.23 | 0.0827 |
| BSA | 0.22 | 0.18, 0.27 | < 0.0001 | 5.82 | 4.82, 6.83 | < 0.0001 |
| Model summary | R2= 0.2256 | < 0.0001 | R2= 0.2905 | < 0.0001 | ||
| Age | 0.06 | 0.03, 0.09 | 0.0002 | 0.14 | −0.63, 0.91 | 0.7193 |
| Female gender | −0.28 | −0.34, −0.22 | < 0.0001 | −8.07 | −9.61, −6.52 | < 0.0001 |
| BMI | 0.20 | 0.17, 0.23 | < 0.0001 | 4.01 | 3.20, 4.81 | < 0.0001 |
| Model summary | R2= 0.2647 | < 0.0001 | R2= 0.2620 | < 0.0001 | ||
| Age | 0.04 | 0.01, 0.08 | 0.0186 | 0.08 | −0.73, 0.88 | 0.8477 |
| Female gender | −0.29 | −0.40, −0.19 | < 0.0001 | −4.70 | −7.07, −2.32 | 0.0001 |
| Height | 0.04 | −0.01, 0.10 | 0.1151 | 3.29 | 2.09, 4.49 | < 0.0001 |
| Model summary | R2= 0.1223 | < 0.0001 | R2= 0.1968 | < 0.0001 | ||
For LAV, models incorporating body size, age, and gender accounted for 19% to 29% of the variability in LAV. Similar to LAD, models using BSA and BMI had the highest R2values. Age was not associated with LAV, when gender and body size measures were controlled. When adjusting for body size using BMI or height, gender had a highly significant association with LAV. This was not true, however, when BSA was used to adjust for body size.
Both LAV and LAD were strongly associated with body size. For those cardiac structural parameters associated with body size, reference values are customarily reported corrected for body size by means of indexation. By controlling for body size with indexation to BSA, BMI, and height, the association of LAD and LAV with age and gender was investigated (Table 4). For LAD, age was associated with LAD when indexed to BSA, BMI, or height, and gender remained significant when LAD was indexed to BSA or BMI. For LAV, no significant association with age was present with indexation to BSA, BMI, or height. However, males had significantly larger LAV in all three indexed models.
| LAD/BSA | LAD/BMI | LAD/Ht | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Parameter Estimate* | Confidence Intervals | p Value | Parameter Estimate* | Confidence Intervals | p Value | Parameter Estimate* | Confidence Intervals | p Value | |
| Female gender | 0.13 | 0.09, 0.17 | < 0.0001 | −0.003 | −0.006, 0.000 | 0.04 | −0.0002 | −0.001, 0.0002 | 0.25 |
| Age | 0.06 | 0.04, 0.08 | < 0.0001 | 0.003 | 0.002, 0.005 | < 0.0001 | 0.0004 | 0.0002, 0.001 | 0.0004 |
| Model summary | R2= 0.1106 | < 0.0001 | R2= 0.0284 | < 0.0001 | R2= 0.0172 | 0.0015 | |||
| LAV/BSA | LAV/BMI | LAV/Ht | |||||||
| Female gender | −1.51 | −2.28, −0.73 | 0.0001 | −0.25 | −0.31, −0.19 | 0.0001 | −0.04 | −0.05, −0.03 | 0.0001 |
| Age | 0.28 | −0.11, 0.66 | 0.16 | 0.01 | −0.01, 0.04 | 0.32 | 0.0002 | −0.004, 0.005 | 0.9359 |
| Model summary | R2= 0.0207 | 0.0005 | R2= 0.094 | < 0.0001 | R2= 0.0726 | < 0.0001 | |||
Gender-specific reference ranges for left atrial dimension and volume, with and without indexing, are provided in Table 5.
| Measurement | Gender | Percentile | ||
|---|---|---|---|---|
| 5% | 50% | 95% | ||
| LAD, cm | Female | 2.80 | 3.50 | 4.20 |
| LAD, cm | Male | 3.00 | 3.90 | 4.60 |
| LAD/BSA, cm/m2 | Female | 1.58 | 2.00 | 2.52 |
| LAD/BSA, cm/m2 | Male | 1.49 | 1.88 | 2.30 |
| LAD/BMI, cm/kg per m2 | Female | 0.100 | 0.131 | 0.176 |
| LAD/BMI, cm/kg per m2 | Male | 0.101 | 0.137 | 0.172 |
| LAD/height, cm/cm | Female | 0.017 | 0.022 | 0.026 |
| LAD/height, cm/cm | Male | 0.017 | 0.022 | 0.027 |
| LAV, ml | Female | 23 | 36 | 54 |
| LAV, ml | Male | 29 | 45 | 69 |
| LAV/BSA, ml/m2 | Female | 14 | 21 | 30 |
| LAV/BSA, ml/m2 | Male | 14 | 22 | 33 |
| LAV/BMI, ml/kg per m2 | Female | 0.94 | 1.37 | 2.07 |
| LAV/BMI, ml/kg per m2 | Male | 1.02 | 1.61 | 2.47 |
| LAV/height, ml/cm | Female | 0.144 | 0.226 | 0.333 |
| LAV/height, ml/cm | Male | 0.164 | 0.257 | 0.390 |
Relationship between atrial size and cardiovascular disease in the entire cohort
The association between left atrial size, as defined by quartiles of LAD/BSA or LAV/BSA, and the presence of cardiovascular disease in the entire cohort is shown in Table 6. Atrial size, by either parameter, is significantly associated with the presence of cardiovascular disease. Moreover, the unadjusted accuracy (area under the receiver operating characteristic curve) was similar for each atrial size parameter in relation to cardiovascular disease except for congestive heart failure, where LAV/BSA had significantly better accuracy than LAD/BSA (p = 0.028). However, when adjusting for age and gender, LAV/BSA had better accuracy than LAD/BSA for hypertension (p = 0.0007), congestive heart failure (p = 0.028), and atrial fibrillation (p = 0.0061).
| Quartile | Unadjusted AUC (95% CI) | Adjusted AUC†(95% CI) | ||||
|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | |||
| LAD/BSA | ||||||
| Hypertension (%) | 21.0 | 25.0 | 33.6 | 39.5 | 0.60 | 0.66† |
| (0.58, 0.63) | (0.64, 0.69) | |||||
| Coronary artery disease (%) | 5.9 | 9.8 | 9.8 | 22.7 | 0.67 | 0.80 |
| (0.63, 0.71) | (0.77, 0.84) | |||||
| Myocardial infarction (%) | 2.6 | 3.9 | 3.5 | 9.3 | 0.65 | 0.80 |
| (0.58, 0.71) | (0.75, 0.84) | |||||
| CHF (%) | 0.4 | 1.2 | 0.4 | 6.5 | 0.83† | 0.85† |
| (0.75, 0.91) | (0.78, 0.92) | |||||
| Valve disease (%) | 0.8 | 1.6 | 2.9 | 11.1 | 0.80 | 0.84 |
| (0.75, 0.86) | (0.80, 0.89) | |||||
| Atrial fib/flutter (%) | 1.2 | 2.0 | 3.7 | 11.3 | 0.77 | 0.83† |
| (0.71, 0.82) | (0.79, 0.88) | |||||
| LAV/BSA | ||||||
| Hypertension (%) | 20.4 | 24.6 | 28.0 | 43.2 | 0.62 | 0.68† |
| (0.59, 0.65) | (0.65, 0.71) | |||||
| Coronary artery disease (%) | 5.3 | 8.3 | 8.7 | 24.8 | 0.70 | 0.81 |
| (0.66, 0.74) | (0.78, 0.84) | |||||
| Myocardial infarction (%) | 1.9 | 3.8 | 3.0 | 10.2 | 0.68 | 0.80 |
| (0.62, 0.75) | (0.76, 0.85) | |||||
| CHF (%) | 0 | 0.6 | 0.6 | 6.8 | 0.88† | 0.89† |
| (0.83, 0.94) | (0.84, 0.95) | |||||
| Valve disease (%) | 1.3 | 1.1 | 2.1 | 11.7 | 0.80 | 0.86 |
| (0.75, 0.86) | (0.82, 0.91) | |||||
| Atrial fib/flutter (%) | 1.1 | 1.7 | 2.3 | 13.6 | 0.80 | 0.86† |
| (0.75, 0.85) | (0.82, 0.90) | |||||
Prevalence of left atrial enlargement in the population
If left atrial enlargement is defined as LAV/BSA >95th percentile in normal subjects, the prevalence of left atrial enlargement in the Olmsted County, Minnesota, population was equal in men and women at 16% (CI, 14% to 19% for both). The prevalence of left atrial enlargement by LAD/BSA was 18% in men and 12% in women (CI, 15% to 20% and 10% to 14%, respectively). The correspondence between the two methods of defining left atrial enlargement is shown in Table 7. Overall, there was 88% observed concordance. However, this observed agreement was heavily influenced by the large number of subjects without left atrial enlargement. The Cohen kappa statistic was 0.54 (CI, 0.49 to 0.59), indicating only fair agreement. The Spearman correlation between the two indexes was 0.65 (p < 0.001). When left atrial enlargement was defined by either index, the odds ratio for the presence of cardiovascular disease with left atrial enlargement was similar (Table 8).
| Subjects, No. (n = 1,886) | ||
|---|---|---|
| LAD/BSA Normal | LAD/BSA Abnormal | |
| LAV/BSA normal | 1,474 | 104 |
| LAV/BSA abnormal | 127 | 181 |
| Cardiovascular Disease | LAD/BSA | LAV/BSA | ||
|---|---|---|---|---|
| LAE, % | Odds Ratio (95% CI) | LAE, % | Odds Ratios (95% CI) | |
| Hypertension | 22 | 2.1 | 27 | 2.7 |
| No hypertension | 12 | (1.7, 2.8) | 12 | (2.1, 3.5) |
| Coronary artery disease | 38 | 4.6 | 38 | 4.0 |
| No coronary artery disease | 12 | (3.4, 6.2) | 13 | (3.0, 5.5) |
| Congestive heart failure | 71 | 15.8 | 74 | 15.7 |
| No congestive heart failure | 14 | (8.0, 31.3) | 15 | (7.6, 32.8) |
| Valve disease | 59 | 9.5 | 61 | 9.4 |
| No valve disease | 13 | (6.0, 15.2) | 14 | (5.8, 15.2) |
| Atrial fib/flutter | 54 | 7.8 | 56 | 7.7 |
| No atrial fib/flutter | 13 | (5.1, 12.1) | 14 | (4.9, 12.0) |
Discussion
A simple and feasible method to measure LAV was applied in a cross-sectional sample of the population and compared with the standard index of left atrial size, LAD. In a subgroup of subjects without cardiovascular disease or cardiac dysfunction (n = 767), both indexes of left atrial size increased with increasing body size and were larger in men. The variability in body size, age, and gender explained up to 29% of the variability of left atrial size in the reference subjects. When the association between left atrial size and body size was controlled for by indexing to BSA, BMI, or height, each indexed variable differed between men and women, except LAD/height. In the reference subjects, there was a positive association between indexed LAD and age, although the magnitude of the change with age was not clinically relevant. There was no association between age and indexed or nonindexed LAV in the reference subjects. In the entire population-based cohort, the prevalence of cardiovascular disease increases with increasing LAD/BSA and LAV/BSA. When adjusted for age and gender, LAV/BSA exhibited a stronger association with cardiovascular disease than LAD/BSA. Left atrial enlargement was common in the general population older than age 45 years, and the prevalence of left atrial enlargement in the population was somewhat higher when LAV/BSA was used to assess left atrial size. The agreement between left atrial enlargement as defined by LAV/BSA and LAD/BSA was only fair. However, left atrial enlargement as defined by either index was associated with a similar prevalence of cardiovascular disease.
LAV
Left atrial size, as measured by a single M-mode dimension, is associated with the presence of cardiovascular disease and is predictive of stroke, atrial fibrillation, and death (1,2). It has been proposed that the left atrium enlarges asymmetrically; hence, LAV, an index that encompasses multiplanar measurements, may be a more accurate measure of atrial size. Although others have used the four-chamber area-length and biplane Simpsons methods to measure LAV (3,18,19), we used an elliptical model (12,20)that incorporates two short-axis and one long-axis measurement and does not require endocardial tracing or complex calculations. Our median normal LAV/BSA values, 21 ml/m2for women and 22 ml/m2for men, are similar to the mean values reported for both genders by using the biplane Simpsons method (20 ± 6 ml/m2) and the four-chamber area-length method (21 ± 7 ml/m2) in 48 normal volunteers by Wang et al. (18). The mean value reported by Tsang et al. (21)using the biplane Simpsons method (22 ± 4 ml/m2) in 138 subjects with otherwise normal cardiac structure and function is also similar to our data. We also confirm that LAV/BSA, when adjusted for age and gender, correlates better than LAD/BSA with the presence of cardiovascular disease. These data suggest that this simple method yields values that are similar to more complex methods of measuring LAV and reflects left atrial remodeling associated with cardiovascular disease. The large number of prospectively studied, rigorously selected reference subjects and the population-based setting used in the current study provide an appropriate venue for the definition of “normal” reference values.
Although LAV is purported to be a superior method to assess left atrial size, the optimal way to account for the association between body size and LAV when reporting LAV has not been established (22). Further, the need to account for gender or age in the definition of upper normal values is not clear from current literature. In the small volunteer group in which normal values were previously described for LAV, predominantly young subjects were studied, and the number of subjects was insufficient to determine if LAV varied with age, gender, or body size (18). The Framingham study (23)indicated that LAD increased with increasing body size and that BMI correlated with LAD more strongly than weight or BSA. Yet, the data are typically presented indexed to height, considered an intrinsic variable of body size that attempts to avoid problems associated with overcorrection for the effect of obesity on body size (24,25). In the current study, models incorporating BSA accounted for more of the variability in LAV in normal subjects, suggesting that indexing to BSA is an appropriate way to control for body size when reporting LAV.
When considering the relationship between body size and LAV in the reference cohort, we did not exclude subjects who were obese if there was no known cardiovascular disease or cardiac dysfunction. The relationship between body size and LAV was stronger for body size indexes that incorporate weight (BMI and BSA), as previously described by Gottdiener et al. (26). Obese subjects free of cardiovascular disease have larger (nonindexed) LAD (27), and weight loss is associated with a decrease in LAD (28). Increases in stroke volume and cardiac output are needed to meet the higher metabolic demands in obese subjects who have larger blood volumes and left ventricular mass than nonobese subjects (27). Indeed, nonobese athletes have similar physiologic changes due to exercise and also have larger atrial size (18,29). Although our reference values are influenced by inclusion of overweight and obese individuals, LAV/BSA was similar in lean (BMI ≤28 kg/m2) and overweight or obese (BMI >28 kg/m2) normal subjects. Prospective follow-up of this cohort may allow us to determine whether the slightly larger LAV observed in an obese individual reflects physiology or is an indicator of covert cardiovascular disease. Indexing left atrial size variables to body size permits more uniform comparison among subjects and may allow more accurate selection of those with atrial enlargement related to cardiovascular abnormalities.
Others (30–32)have reported that LAD increases slightly with age. In our study, age was significantly associated with LAD in the multivariate analysis. However, the increment in LAD/BSA associated with an eight-year increase in age was small (0.07 cm/m2) and is not likely to be clinically relevant. In contrast, our data and that of others suggest that increasing age is not associated with an increase in LAV/BSA when excluding or controlling for the presence of cardiovascular disease (12,18).
In general, gender and body size are related. In the multivariable analysis, the model combining age, gender, and BSA suggested that gender was not independently associated with LAV. However, when controlling for body size by simply indexing LAV to BSA, we find a small but significant difference between LAV/BSA in men and women, suggesting the need for gender-specific reference values for LAV/BSA.
Association of LAV and cardiovascular disease
The traditional index of left atrial size, LAD, tends to be larger in those individuals with cardiovascular disease (1,2). This association likely reflects left atrial pressure and volume overload in response to cardiac dysfunction associated with cardiovascular diseases. The relationship between LAD and the presence of atrial fibrillation is also well established (33). As expected, in the current study, the prevalence of cardiovascular diseases increased with increasing LAV/BSA. The association between cardiovascular disease and LAV/BSA was stronger than that observed with LAD/BSA after adjustment for age and gender.
Prevalence of left atrial enlargement in the population
As defined by LAD or LAV, the prevalence of left atrial enlargement in this middle-aged to elderly segment of the population was significant: 16% in men and women by using LAV/BSA and 18% (men) and 12% (women) by using LAD/BSA. The high prevalence of left atrial enlargement reflects the prevalence of cardiovascular disease in this community-based population aged ≥45 years in which 29.5% had hypertension, 4.8% have had a myocardial infarction, 2.2% had heart failure, 7.5% had diabetes, and 2.0% have had a stroke. These data are important because the Framingham study has established that left atrial size predicts development of atrial fibrillation, stroke, and death in a community-based population. It remains unclear whether subjects with left atrial enlargement should be targeted for more aggressive intervention, as are patients with hypertension or diabetes and target organ damage.
These cross-sectional data do not allow us to establish that LAV is a better index of left atrial enlargement. Lester et al. (3)suggested that the left atrium may become less spherical as it enlarges and, thus, that LAV may be a more sensitive index of left atrial enlargement. Indeed, Tsang et al. (33)reported that LAV was more strongly associated than LAD with the future development of atrial fibrillation in a large clinical population. Although the prevalence of cardiovascular disease was similar among those with left atrial enlargement as defined by LAV and LAD, LAV identified a slightly larger population with left atrial enlargement, and the agreement between the two indexes, as defined by the kappa statistic, was only fair. These data suggest that the two indexes identify somewhat different segments of the population as abnormal. Thus, the potential exists for LAV to be a more powerful predictor of future cardiovascular events within the population, but it will require large longitudinal studies in which standardized increments in LAD and LAV are compared for their predictive value.
In conclusion, our study describes a simple and highly feasible method to quantify LAV, establishes the contribution of body size, gender, and age to LAV, provides normal values for the index in a rigorously defined, population-based reference population, and confirms the association of LAV measured in this way with cardiovascular disease. Although more time-consuming methodologies for measuring LAV have been suggested, our data should enable echocardiographic laboratories to incorporate this simple and standardized measurement into their practice. We also establish that left atrial enlargement is common in the community and reflects the extent of cardiovascular disease in those older than age 45 years.
1. : "Echocardiographic predictors of nonrheumatic atrial fibrillation: the Framingham Heart study". Circulation 1994; 89: 724.
2. : "Left atrial size and the risk of stroke and death: the Framingham Heart study". Circulation 1995; 92: 835.
3. : "Best method in clinical practice and in research studies to determine left atrial size". Am J Cardiol 1999; 84: 829.
4. : "Left atrial volume estimation by two-dimensional echocardiography". Cathet Cardiovasc Diagn 1981; 7: 165.
5. : "Left atrial volume calculation by angiocardiography in children". Chest 1973; 63: 189.
6. : "The patient record in epidemiology". Sci Am 1981; 245: 54.
7. : "History of the Rochester Epidemiology Project". Mayo Clin Proc 1996; 71: 266.
8. : "The sixth report of the Joint National Committee on prevention, detection, evaluation, and treatment of high blood pressure". Arch Intern Med 1997; 157: 2413.
9. : "International diagnostic criteria for acute myocardial infarction and acute stroke". Am Heart J 1984; 108: 150.
10. : "The natural history of congestive heart failure: the Framingham study". N Engl J Med 1971; 285: 1441.
11. : "Recommendations regarding quantitation in M-mode echocardiography: results of a survey of echocardiographic measurements". Circulation 1978; 58: 1072.
12. : "Quantitative angiocardiography. II. The normal left atrial volume in man". Circulation 1968; 37: 800.
13. : "Recommendations for quantitation of the left ventricle by two-dimensional echocardiography: American Society of Echocardiography Committee on Standards, Subcommittee on Quantitation of Two-Dimensional Echocardiograms". J Am Soc Echocardiogr 1989; 2: 358.
14. : "A new, simplified and accurate method for determining ejection fraction with two-dimensional echocardiography". Circulation 1981; 64: 744.
15. : "Evaluation of diastolic filling of left ventricle in health and disease: Doppler echocardiography is the clinician’s rosetta stone". J Am Coll Cardiol 1997; 30: 8.
16. : "Clinical utility of Doppler echocardiography and tissue Doppler imaging in the estimation of left ventricular filling pressures: a comparative simultaneous Doppler-catheterization study". Circulation 2000; 102: 1788.
17. : "Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach". Biometrics 1988; 44: 837.
18. : "Atrial volume in a normal adult population by two-dimensional echocardiography". Chest 1984; 86: 595.
19. : "Noninvasive quantitation of the left heart by echocardiography and scintigraphy". Cardiovasc Clin 1986; 17: 45.
20. : "The relationship of left atrial pressure and volume in patients with heart disease". Am Heart J 1964; 67: 635.
21. : "Left ventricular diastolic dysfunction as a predictor of the first diagnosed nonvalvular atrial fibrillation in 840 elderly men and women". J Am Coll Cardiol 2002; 40: 1636.
22. : "Interpretation of echocardiographic measurements: a call for standardization". Am Heart J 2000; 139: 412.
23. : "Influence of blood pressure on left atrial size: the Framingham Heart study". Hypertension 1995; 25: 1155.
24. Levy D, Anderson KM, Savage DD, Kannel WB, Christiansen JC, Castelli WP. Echocardiographically detected left ventricular hypertrophy: prevalence and risk factors: the Framingham Heart study. Ann Intern Med 1988;108:7–13
25. Vasan RS, Larson MG, Levy D, Evans JC, Benjamin EJ. Distribution and categorization of echocardiographic measurements in relation to reference limits: the Framingham Heart study: formulation of a height- and sex-specific classification and its prospective validation. Circulation 1997;96:1863–73
26. : "Left atrial size in hypertensive men: influence of obesity, race and ageDepartment of Veterans Affairs Cooperative Study Group on Antihypertensive Agents". J Am Coll Cardiol 1997; 29: 651.
27. : "Left atrial enlargement in healthy obese: prevalence and relation to left ventricular mass and diastolic function". Can J Cardiol 1996; 12: 257.
28. : "Assessment of cardiac function in patients who were morbidly obese". Surgery 1990; 108: 809.
29. : "Echocardiographic features of left atrium in elite male athletes". Am J Cardiol 1996; 78: 1314.
30. : "Echocardiographic measurements in normal subjects: evaluation of an adult population without clinically apparent heart disease". J Clin Ultrasound 1979; 7: 439.
31. : "Normal adult cross-sectional echocardiographic values: linear dimensions and chamber areas". Echocardiography 1984; 1: 403.
32. : "Left atrial mechanical function in the healthy elderly: new insights from a combined assessment of changes in atrial volume and transmitral flow velocity". J Am Soc Echocardiogr 1995; 8: 801.
33. : "Left atrial volume: important risk marker of incident atrial fibrillation in 1655 older men and women". Mayo Clin Proc 2001; 76: 467.
Abbreviations
| BMI | body mass index |
| BSA | body surface area |
| CI | confidence interval |
| EF | ejection fraction |
| LAD | left atrial dimension |
| LAV | left atrial volume |
| 2D | two-dimensional |
Footnotes
☆ Supported by grants from the Public Health Service (NIH HL 55502 and NIH AR 30582), the Marriott Foundation, the Miami Heart Research Institute, and the Mayo Foundation.
{kind=link}