Detection of viruses in myocardial tissues by polymerase chain reaction: evidence of adenovirus as a common cause of myocarditis in children and adults
Clinical study
Abstract
Objectives:
The purpose of this study was to analyze cardiac tissue and blood for viral genomes using polymerase chain reaction (PCR) to define the common viral etiologies of myocarditis by age group.
Background:
Enteroviruses are considered the most common cause of myocarditis at all ages. Diagnosis relies on viral cultures, serology, and cardiac histology, which lack sensitivity, as well as PCR. However, in many cases enteroviruses are not detected.
Methods:
Cardiac samples were obtained for PCR analysis from patients with myocarditis (n = 624) and dilated cardiomyopathy (DCM) (n = 149). Patients were analyzed by age group, including neonates (n = 116), infants (n = 191), toddlers (n = 87), children (n = 110), adolescents (n = 92), and adults (n = 177). After nucleic acids had been extracted from an endomyocardial biopsy, an explant, or autopsy samples, PCR and reverse transcription PCR were performed to detect the genomic sequences of enterovirus, adenovirus, cytomegalovirus (CMV), herpes simplex virus (HSV), Epstein-Barr virus (EBV), parvovirus, respiratory syncytial virus (RSV), and influenza A virus.
Results:
Viral genome was amplified (adenovirus = 142, enterovirus = 85, CMV = 18, parvovirus = 6, influenza A = 5, HSV = 5, EBV = 3, RSV = 1) from 239 (38%) of the 624 samples from myocarditis patients, including 26 patient samples in which dual infection was found. Virus was detected in 30 (20%) of 149 DCM patient samples; only adenovirus (n = 18) and enterovirus (n = 12) were detected.
Conclusions:
Polymerase chain reaction identified adenovirus as the most common virus in the myocardium of children and adults with myocarditis and DCM. Although enteroviruses are also found in these patients, they appear to be a less common cause of myocarditis than adenovirus.
Introduction
Viral infections of the heart are important causes of morbidity and mortality in children and adults. Acute myocarditis typically presents with severe clinical manifestations, especially in the newborn period (1). Idiopathic dilated cardiomyopathy (DCM) appears to occur as a late sequela of acute or chronic viral myocarditis (2,3), either due to persistence of virus (4)or to an autoimmune phenomenon occurring secondary to previous exposure to the inciting virus (5). The affected individual may require long-term medical therapy for congestive heart failure (CHF) and, in many cases, orthotopic heart transplantation (OHT). In some cases, sudden cardiac death occurs (6), particularly in athletes (7).
Enteroviruses, and especially the Coxsackievirus B family, have been considered the most common cause of acute myocarditis. Viral diagnosis has classically been based on identification of virus by peripheral culture methods and/or serial serology (2,8); isolation of virus from myocardium is usually unsuccessful, however. Endomyocardial biopsy (EMB) and histopathologic assessment were developed to improve diagnostic capabilities, but they were inconsistent among pathologists. It was hoped that the “Dallas” criteria (9)would improve the high rate of diagnostic disagreement by establishing uniform criteria. However, because of insensitivity (10)and possible risks involved in biopsies, particularly in small or critically ill children, many centers abandoned EMB as a diagnostic tool.
The ability to diagnose viral infection in the cardiac tissue of patients with myocarditis and DCM improved with the advent of molecular hybridization by Bowles et al. (4,11). These studies also led to the hypothesis that DCM was caused by enteroviral persistence and supported the view that DCM is a late sequela of viral myocarditis. More recently, polymerase chain reaction (PCR) has been employed in the rapid detection of viral sequences in many tissues and body fluids, including Coxsackievirus-specific ribonucleic acid (RNA) in the myocardium of patients with suspected myocarditis or DCM (12–15). Evidence from our laboratory suggested that adenovirus is a commonly associated viral genome found in hearts of affected children and could be an important cause of myocarditis and DCM (16–18). The purpose of this study was to analyze the etiologic agents potentially responsible for myocarditis and DCM in different age groups.
Methods
Clinical diagnostic criteria
Clinical diagnostic criteria
Inclusion criteria for the study included initial presenting symptoms of acute cardiovascular collapse, acute CHF with or without ventricular tachycardia, and evidence of cardiac dysfunction using noninvasive methods.
Echocardiographic criteria used in the diagnosis of acute myocarditis or chronic cardiomyopathy included left ventricular (LV) dysfunction and ventricular dilation calculated from M-mode echocardiograms (19). Doppler and color Doppler were used to determine atrioventricular valve regurgitation.
After cardiac catheterization and EMB, up to nine biopsy specimens (1.8 mm3or 2.2 mm3) were fixed in formalin for histology, glutaraldehyde for electron microscopy, and cold viral media for culture, with one or two samples either snap-frozen in liquid nitrogen or formalin-fixed for PCR analysis. All explanted hearts were sampled (right ventricle [RV] and LV) and snap-frozen within 10 min of explantation. All autopsies were performed in standard fashion; LV and RV wedges were frozen, formalin-fixed, or paraffin-embedded. All histologic results were based on the “Dallas” criteria (9). The presumptive diagnosis of myocarditis was based on histopathologic criteria of definite or borderline myocarditis on biopsy using the “Dallas” criteria or a clinical diagnosis of acute-onset heart failure (new-onset dyspnea with associated hepatosplenomegaly, physical exam findings of reduced cardiac output and gallop rhythm, and evidence of DCM on chest X-ray or echocardiography) with history of recent viral illness. In cases where chronic myopathic changes were identified on histology, the diagnosis of DCM was favored in the absence of significant inflammation. All studies on humans were performed in accordance with local institutional review board regulations.
Exclusion criteria
All children with the diagnosis of anomalous left coronary artery from the pulmonary artery, Kawasaki disease, adriamycin-induced cardiomyopathy, critical neonatal aortic stenosis, or postoperative congenital heart disease repair were excluded. Adults with evidence of alcohol-induced cardiomyopathy, peripartum cardiomyopathy, adriamycin-induced cardiomyopathy, or ischemic cardiomyopathy were also excluded. All patients previously published were excluded from this study.
Patient samples
Myocardial samples from 773 patients with myocarditis and DCM enrolled in 20 institutions in the U.S. were studied. All local patients (Texas Children’s Hospital) were obtained consecutively, but samples from other centers were selected on the basis of the clinical judgment of the cardiologist. Sample sources included 357 RV EMB, 234 autopsy, and 182 specimens from explanted hearts. Myocardial samples were collected from 165 age-matched children and 50 adults undergoing OHT (n = 109) or autopsy (n = 106). None of the patients evaluated in this study has previously been published.
Evaluation for infection
Blood (n = 301 samples), nasopharyngeal (n = 189), urine (n = 114), and stool (n = 82) samples were obtained when possible and cultured for virus (total patients cultured = 333). Serial serology for virus was obtained when possible (n = 452). Endomyocardial biopsies were cultured for virus (n = 96) and also evaluated for viral particles by electron microscopy (n = 206). Post-mortem cardiac cultures were performed in 109 patients. Viral cultures were performed using standard virologic techniques, as previously described (16,17).
Template preparation and PCR
Total RNA and deoxyribonucleic acid were isolated simultaneously from frozen, formalin-fixed tissue (1.8 to 3.0 mm3) or from paraffin-embedded tissue sections, using a modification of the RNAzol method, as previously described (16–18). Paraffin-embedded tissue was first extracted with xylene (two times) then washed in ethanol to remove the paraffin before homogenization in RNAzol. Nucleic acids isolated from cultures or tissues infected with Adenovirus Type 5, Coxsackievirus B4, cytomegalovirus (CMV) strain AD169, herpes simplex virus (HSV) Type 1, parvovirus B19, Epstein-Barr virus (EBV), or influenza virus type A were used as positive controls.
For the detection of the enteroviruses, respiratory syncytial virus (RSV), and influenza viruses (RNA viruses), reverse transcriptase PCR was employed, whereas for adenovirus, CMV, HSV, parvovirus, and EBV (deoxyribonucleic acid viruses), PCR was utilized (16–18).
All samples were analyzed without knowledge of the clinical, culture, or serologic data and were performed in duplicate. Verification of the presence of amplifiable nucleic acid extracted from each sample was performed by amplification of cellular nucleic acid (K-ras or beta-actin).
Statistical analysis
We compared frequencies of virus detection among myocarditis, DCM, and control groups by chi-square analysis.
Results
Patient population
Patient population
Patients with a clinical picture or hospital course consistent with the diagnosis of acute myocarditis or DCM, presenting between January 1988 and January 2000, in whom cardiac tissue and histology were available, were analyzed. A total of 773 patients met this initial inclusion criteria; ages ranged from one day to 42 years (mean age = 6.2 years; median age = 13 years). The patients were divided into groups based on age: neonates (age 1 day to 1 month, n = 116), infants (age 1 month to 1 year, n = 191), toddlers (age 1 year to 5 years, n = 87), children (age 5 years to 13 years, n = 110), adolescents (age 13 years to 18 years, n = 92), and adults (age above 18 years, n = 177). A total of 165 children and 50 adults with medical histories inconsistent with these criteria were included as unaffected, age-matched control patients (described later).
Clinical presentation
Of 773 affected individuals evaluated, myocarditis was diagnosed in 624 and DCM in the remainder (n = 149). Patients presented with acute cardiovascular collapse (n = 247), new-onset CHF (n = 381), respiratory distress (n = 83), or ventricular tachycardia (n = 62). Only 44 of the 624 patients with myocarditis did not have a history consistent with a preceding viral illness. In the 149 patients with DCM, 12 had histories indicative of viral infection.
The 165 control patients included 123 individuals with congenital heart disease, 42 individuals with hypertrophic cardiomyopathy, and 50 trauma victims. None had a history of recent viral illness or histologic evidence of myocarditis.
Prognosis
The overall prognosis of the 624 patients with acute myocarditis studied was poor, with an overall mortality of 51% (318 of 624). In the 149 DCM patients, 61 underwent OHT; one of these patients expired two months post transplantation from disseminated CMV infection, and the autopsy specimen was analyzed by PCR. The majority of patients with myocarditis (430 of 624) had poor recovery of their cardiac function (including all 318 of the deaths), whereas the remaining patients had either mild recovery with persistence of depressed cardiac function (89 of 624), complete recovery (93 of 624), undergone transplantation (121 of 624), or remained critically ill awaiting OHT (3 of 624). None of the “control” patients had history of recent viral illness or signs and symptoms of acute cardiomyopathy. When analyzed by age group, differences in outcome were notable between groups (Table 1), as described below: for neonates, 78 of 116 (67%) deaths, 12 of 116 (10%) persistently depressed functions, and 26 of 116 (23%) improved; for infants, 108 of 191 (55%) deaths, 26 of 191 (12%) persistently depressed function, and 65 of 191 (32%) improved; for toddlers, 19 of 87 (22%) deaths, 28 of 87 (32%) persistently depressed function, and 40 of 87 (46%) improved; for children, 28 of 110 (25%) deaths, 15 of 110 (14%) persistent dysfunction, and 67 of 110 (61%) improved; for adolescents, 18 of 92 (20%) deaths, 12 of 92 (13%) persistently depressed function, and 62 of 92 (67%) improved; for adults, 67 of 177 (38%) deaths, 19 of 177 (11%) persistently depressed function, and 91 of 177 (51%) improved.
| Age | Diagnosis | # Patients | Death | Transplant | Persistent DCM | Improved |
|---|---|---|---|---|---|---|
| Newborn | Myocarditis | 93 | 78 | 13 | 12 | 26 |
| (n = 116) | DCM | 23 | 3 | 4 | 12 | 4 |
| Infants | Myocarditis | 152 | 108 | 16 | 26 | 65 |
| (n = 191) | DCM | 39 | 7 | 12 | 11 | 9 |
| Toddlers | Myocarditis | 69 | 19 | 9 | 28 | 40 |
| (n = 87) | DCM | 18 | 3 | 4 | 5 | 6 |
| Children | Myocarditis | 90 | 28 | 21 | 15 | 67 |
| (n = 110) | DCM | 20 | 3 | 6 | 6 | 5 |
| Adolescents | Myocarditis | 76 | 18 | 16 | 12 | 62 |
| (n = 92) | DCM | 16 | 5 | 6 | 3 | 2 |
| Adults | Myocarditis | 144 | 67 | 46 | 19 | 91 |
| (n = 177) | DCM | 33 | 4 | 19 | 2 | 8 |
Serology/cultures
Significant neutralizing titers were detected in 152 of the 452 (38%) patients studied (46 enterovirus, 12 adenovirus, 42 CMV, 9 HSV, 3 EBV, 7 parvovirus, 14 influenza, 19 RSV) using acute and convalescent titers. Virus was cultured from peripheral samples from 107 of 333 patients (38 enterovirus, 23 adenovirus, 28 CMV, 8 HSV, 2 EBV, 8 influenza), whereas 7 (6%) of 109 patients had positive post-mortem viral cultures. Four of these patients had post-mortem positive cultures for enterovirus from heart, brain, liver, and kidney, and three patients grew adenovirus from the lungs and heart. Two patients grew CMV from the heart and lungs (one in a patient who grew enterovirus, one in a patient who grew adenovirus). One other child had negative viral cultures, but was noted to have adenoviral-like particles in the heart by electron microscopy.
PCR analysis
Myocarditis
Myocarditis
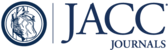
Polymerase chain reaction amplified viral genome in 239 of 624 (38%) samples obtained from patients with myocarditis (Table 2). Among the different types of samples tested, 38% of RV EMB, 25% of explanted tissue, and 53% of autopsy samples were positive. Of the 239 positive PCR samples, 142 were positive for adenovirus (Fig. 1), 85 for enterovirus, 18 for CMV, six for parvovirus, five for influenza A, five for HSV Type 1, three for EBV, and one for RSV, including 26 samples that were positive for two viruses (6 with adenovirus and CMV, 6 with enterovirus and CMV, and 14 with adenovirus and enterovirus). Sequence analysis of adenovirus amplimers identified adenovirus type 2 in about 80% and type 5 in the remainder, except for type 6 in one sample.
| Diagnosis | # Samples | # of Samples PCR+ | PCR Amplimer (#)* |
|---|---|---|---|
| Myocarditis | 624 | 239 (38%) | Adenovirus 142 (23%) |
| Enterovirus 85 (14%) | |||
| CMV 18 (3%) | |||
| Parvovirus 6 (<1%) | |||
| Influenza A 5 (<1%) | |||
| HSV 5 (<1%) | |||
| EBV 3 (<1%) | |||
| RSV 1 (<1%) | |||
| DCM | 149 | 30 (20%) | Adenovirus 18 (12%) |
| Enterovirus 12 (8%) | |||
| Total | 773 | 269 (35%) | |
| Controls | 215 | 3 (1.4%) | Enterovirus 1 (<1%) |
| CMV 2 (<1%) |

(Left)A nine-month-old (TT) presented with a one-day history of fever, irritability, poor feeding, respiratory distress, and poor ventricular function by echocardiography. Death ensued within four hours of presenting to the emergency room. Formalin-fixed cardiac tissue (TTRV1) was positive for adenovirus by polymerase chain reaction (PCR), as demonstrated by the 308 bp PCR product—the same size seen with the adenovirus type 5 control. The 135 bp band is the k-ras PCR product. Note that Patient ALH’s right ventricular endomyocardial biopsy was negative for the adenoviral PCR product but amplifies the 135 bp k-ras product. (Right)Southern blot and hybridization with a radiolabeled adenovirus probe.
Of 107 patients with positive peripheral cultures, 86 (80%) amplified viral genome by PCR with 76% agreement in the results (66 of 86). Polymerase chain reaction analysis of blood obtained from 300 patients at the same time that tissue was obtained amplified virus in just three (CMV in 2, enterovirus in 1). In all age groups, adenovirus was most commonly detected, with enteroviruses second-most common (Fig. 2).

Number of myocarditis patients by age group, positive for viruses by polymerase chain reaction. CMV = cytomegalovirus; EBV = Epstein-Barr virus; HSV = herpes simplex virus; RSV = respiratory syncytial virus.
Dilated cardiomyopathy
In 149 patients with DCM (63 RV EMB, 25 autopsy, 61 explants), 30 myocardial samples (20%) were positive for viral genome (Table 2). Eighteen (60%) of the PCR-positive samples were positive for adenovirus, with the remainder enterovirus (Fig. 3). None of the blood samples from these patients was PCR-positive.

Number of dilated cardiomyopathy patients by age group, positive for viruses by polymerase chain reaction. Black bars= adenovirus; lined bars= enterovirus.
Controls
Of the 215 “control” samples, just three (1.4%) amplified virus: enterovirus from one and CMV from two (Table 2).
Histopathology
In the 624 patients with a clinical diagnosis of myocarditis, histopathology was consistent with acute myocarditis in 409 (66%), whereas the remaining 215 were considered borderline myocarditis and had a history of recent viral illness. Whereas 67 (79%) of the 85 enterovirus-positive cases had acute myocarditis by histology, only 57 (40%) of the 142 adenovirus-positive cases had similar findings, indicating that adenovirus infection is significantly associated with less inflammation than enterovirus infection (p ≤ 0.01).
Histology in patients with DCM demonstrated borderline or mild findings of inflammatory infiltrates in 16 of 149 cases (10%) in the face of chronic myopathy changes, whereas the remaining 133 patients (90%) had histology typical only of DCM. Significantly, in 11 (69%) of the 16 patients with inflammatory infiltrates, virus was detected, compared with just 19 (14%) of the patients without inflammation (p ≤ 0.01). Of the 11 DCM patients with inflammatory infiltrates, nine were positive for enterovirus and two were positive for adenovirus. Thus, there was a statistically significant difference (p ≤ 0.01) between the degree of inflammation in the enterovirus positive samples (9 of 12 = 75%) compared with the adenovirus samples (2 of 18 = 11%).
Discussion
Enteroviruses have been considered responsible for up to 50% of cases of acute myocarditis and for some cases of DCM due to persistent viral infection (4,11–14,20). In this report, we demonstrate adenoviruses to be significant causes of myocarditis in both children and adults. However, this should not be surprising. In 1958, Chany et al. (21)reported 23 patients with adenoviral pneumonia, eight ending in fatality. Two of these children had associated myocarditis, both due to adenovirus type 7a. Other reports of myocarditis with adenoviral pneumonia have also been described (22). Similarly, Henson and Mufson (23)reported an 11-month-old child with myocarditis and interstitial pneumonitis due to adenovirus type 21. Gardiner and Short (24)studied 60 patients with acute myocarditis or pericarditis, finding evidence of specific infection in only 18 patients, including Coxsackievirus B in nine, adenovirus in two, and influenza in two. Berkovich et al. (25)studied 12 children with myocarditis; eight had laboratory evidence of recent viral infection, and viral agents were isolated in five children. Of these, two had adenovirus isolated from stool samples (types 1 and 2), whereas three children had enterovirus (Coxsackievirus B2, B5, and Echovirus 11). In one child with adenovirus, a pathologic diagnosis of endocardial fibroelastosis (EFE) was made, possibly because of in utero myocarditis as a consequence of transplacental viral infection. Recently, adenoviral myocarditis in fetuses with non-immune hydrops was reported (26,27), supporting adenovirus as a possible cause of in utero heart disease. In addition, studies in our laboratory (16,17,26,27)and others (28)have shown adenoviral genome to be common within the myocardium of children with myocarditis or DCM, whereas Pauschinger et al. (18)found adenovirus and enterovirus in adults with LV dysfunction.
In the study presented here, analysis of a large number of samples identified adenoviral genome frequently in the myocardium of patients with myocarditis of DCM (more frequently than enteroviruses). However, because some of the samples analyzed were formalin-fixed, it is possible that the sensitivity of enteroviral RNA detection was reduced, and a slightly lower rate of detection of the enteroviruses was noted in fixed versus frozen samples, although this did not reach statistical significance. Further, we have previously reported studies of the detection of RNA viruses in fixed tissue (17,29). None of the children (affected or controls) was receiving immunosuppression and no difference in the occurrence of routine infections was noted between controls and affected children, supporting the cause-and-effect hypothesis for the detection of viruses in the myocardium. Interestingly, as we previously reported (16), histologic analysis demonstrates that adenovirus-positive patients typically have mild or borderline myocarditis by the “Dallas” criteria, whereas enteroviruses are more commonly associated with acute myocarditis as well as the presence of inflammatory infiltrates in the DCM patients. This is a likely reason that the adenoviruses have been overlooked as significant causes of myocarditis over the years.
The question of whether adenoviruses are indeed a cause of myocarditis in children and adults is further supported by the recent finding of the so-called common Coxsackievirus B-adenovirus receptor (30–32). This receptor binds both group B Coxsackieviruses and the group C adenoviruses, which are reported here and elsewhere to be the most common viruses found in patients with myocarditis or DCM. The discovery of this receptor lends further credence to the idea that adenoviruses not only play a significant role in the etiology of myocarditis and DCM but could also be responsible for the occasional cases of “familial” myocarditis where several family members develop DCM with clinical data suggestive of myocarditis (33). Recently, Noutsias et al. (34)reported the increased expression of Coxsackievirus B-adenovirus receptor in the myocardium of patients with DCM by comparison with normal hearts. Additionally, Badorff et al. (35)reported the identification of Coxsackievirus B3-encoded protease 2A-mediated degradation of dystrophin in the hearts of infected mice leading to disruption of the dystrophin-associated glycoprotein complex. These data support the role of viruses in the development of DCM and suggest a commonality of pathogenesis between the acquired and inherited forms of this disease because mutations in dystrophin, as well as other proteins of the cytoarchitecture, have been shown to cause DCM in humans and animals (36).
The data presented herein could have significant therapeutic consequences. Currently, few pharmacologic agents have been developed for specific viral infections. Although such agents as ribavirin, gancyclovir, and acyclovir have had moderate impact on certain infectious disorders such as RSV pneumonitis and CMV disease in transplanted patients, other therapeutic agents have been slow to develop. Currently no specific therapy is approved for adenovirus or enteroviruses. However, other approaches may be worth considering. We have previously shown that EFE, a major cause of DCM in the young that essentially disappeared by the early 1980s, was caused by mumps virus (29). Based on the chronology of the disappearance of the disease (i.e., beginning of mumps viral vaccination in the years just before the extinction of EFE), it is likely that vaccination was responsible for the impressive decrease in the reported cases of EFE. Specific vaccinations for adenoviruses and enteroviruses could result in diminished numbers of myocarditis and DCM cases, leading to drastic cuts in the number of cardiac transplants and cost of care.
1. : "Acute myocarditis in infancy and childhood". Prog Cardiovasc Dis 1964; 7: 179.
2. : "Active myocarditis in the spectrum of acute dilated cardiomyopathies. Clinical features, histologic correlates, and clinical outcome". N Engl J Med 1985; 312: 885.
3. : "The role of myocarditis in end-stage dilated cardiomyopathy". Tex Heart Inst J 1987; 14: 268.
4. : "End-stage dilated cardiomyopathy. Persistence of enterovirus RNA in myocardium at cardiac transplantation and lack of immune response". Circulation 1989; 80: 1128.
5. Schultheiss HP, Schulze K, Dorner A. Significance of the adenine nucleotide translocator in the pathogenesis of viral heart disease. Mol Cell Biochem 1996;163–64:319–27
6. : "Occurrence of myocarditis in sudden death in children". J Forensic Sci 1977; 22: 188.
7. : "Sudden death in young athletes. Lessons from the Hank Gathers affair". N Engl J Med 1993; 329: 55.
8. : "A six-year study of coxsackievirus B infections in heart disease". J Hyg (Lond) 1974; 73: 165.
9. : "Myocarditis. A histopathologic definition and classification". Am J Cardiovasc Pathol 1987; 1: 3.
10. : "Insensitivity of right ventricular endomyocardial biopsy in the diagnosis of myocarditis". J Am Coll Cardiol 1989; 14: 915.
11. : "Detection of Coxsackie-B-virus-specific RNA sequences in myocardial biopsy samples from patients with myocarditis and dilated cardiomyopathy". Lancet 1986; 1: 1120.
12. : "Detection of enterovirus RNA in myocardial biopsies from patients with myocarditis and cardiomyopathy using gene amplification by polymerase chain reaction". Circulation 1990; 82: 8.
13. : "Detection of enteroviral RNA in idiopathic dilated cardiomyopathy and other human cardiac tissues". J Clin Invest 1992; 90: 156.
14. : "Search for Coxsackievirus B3 RNA in idiopathic dilated cardiomyopathy using gene amplification by polymerase chain reaction". Am J Cardiol 1992; 69: 658.
15. : "Rapid diagnosis of enterovirus infection by magnetic bead extraction and polymerase chain reaction detection of enterovirus RNA in clinical specimens". J Clin Microbiol 1993; 31: 31.
16. : "Acute myocarditis: rapid diagnosis by PCR in children". Circulation 1994; 90: 330.
17. : "Analysis of formalin-fixed and frozen myocardial autopsy samples for viral genome in childhood myocarditis and dilated cardiomyopathy with endocardial fibroelastosis using polymerase chain reaction (PCR)". Cardiovasc Pathol 1995; 4: 3.
18. : "Detection of adenoviral genome in the myocardium of adult patients with idiopathic left ventricular dysfunction". Circulation 1999; 99: 1348.
19. : "Echocardiographic evaluation of left ventricular function in children with congestive cardiomyopathy". Am J Cardiol 1979; 44: 1332.
20. : "In situ detection of enteroviral genomes in myocardial cells by nucleic acid hybridization: an approach to the diagnosis of viral heart disease". Proc Natl Acad Sci U S A 1987; 84: 6272.
21. : "Severe and fatal pneumonia in infants and young children associated with adenovirus infections". Am J Hyg 1958; 67: 367.
22. : "Extracorporeal membrane oxygenation: its role in the survival of a child with adenoviral pneumonia and myocarditis". South Med J 1983; 76: 1171.
23. : "Myocarditis and pneumonitis with type 21 adenovirus infection. Association with fatal myocarditis and pneumonitis". Am J Dis Child 1971; 121: 334.
24. : "Four faces of acute myopericarditis". Br Heart J 1973; 35: 433.
25. : "Virologic studies in children with acute myocarditis". Am J Dis Child 1968; 115: 207.
26. : "Intrauterine adenoviral myocarditis presenting as nonimmune hydrops fetalis: diagnosis by polymerase chain reaction". Pediatr Infect Dis J 1994; 13: 144.
27. : "Detection of intrauterine viral infection using the polymerase chain reaction". Mol Genet Metab 1998; 63: 85.
28. : "Adenovirus myocarditis: retrospective diagnosis by gene amplification from formalin-fixed, paraffin-embedded tissues". Hum Pathol 1994; 25: 831.
29. : "Viral infection of the myocardium in endocardial fibroelastosis. Molecular evidence for the role of mumps virus as an etiologic agent". Circulation 1997; 95: 133.
30. : "Isolation of a common receptor for Coxsackie B viruses and adenoviruses 2 and 5". Science 1997; 275: 1320.
31. : "HCAR and MCAR: the human and mouse cellular receptors for subgroup C adenoviruses and group B coxsackieviruses". Proc Natl Acad Sci U S A 1997; 94: 3352.
32. : "Genomic organization and chromosomal localization of the human Coxsackievirus B-adenovirus receptor gene". Hum Genet 1999; 105: 354.
33. : "Clinical and pathologic findings of myocarditis in two families with dilated cardiomyopathy". Am Heart J 1984; 107: 127.
34. : "Human coxsackie-adenovirus receptor is colocalized with integrins alpha(v)beta(3) and alpha(v)beta(5) on the cardiomyocyte sarcolemma and upregulated in dilated cardiomyopathy: implications for cardiotropic viral infections". Circulation 2001; 104: 275.
35. : "Enteroviral protease 2A cleaves dystrophin: evidence of cytoskeletal disruption in an acquired cardiomyopathy". Nat Med 1999; 5: 320.
36. : "The role of cytoskeletal proteins in cardiomyopathies". Curr Opin Cell Biol 1998; 10: 131.
Abbreviations
| CHF | congestive heart failure |
| CMV | cytomegalovirus |
| DCM | dilated cardiomyopathy |
| EBV | Epstein-Barr virus |
| EFE | endocardial fibroelastosis |
| EMB | endomyocardial biopsy |
| HSV | herpes simplex virus |
| LV | left ventricle/ventricular |
| OHT | orthotopic heart transplantation |
| PCR | polymerase chain reaction |
| RNA | ribonucleic acid |
| RSV | respiratory syncytial virus |
| RV | right ventricle/ventricular |
Footnotes
☆ This work was supported by the Texas Children’s Hospital Foundation Chair in Pediatric Cardiovascular Research; the National Heart, Lung, and Blood Institute, National Institutes of Health; the American Heart Association, Texas Affiliate; the Abercrombie Cardiology Fund of Texas Children’s Hospital; and the Abby Glaser Children’s Heart Fund (Texas Children’s Hospital, Houston, Texas).
{kind=link}
{kind=link}
{kind=link}
Editorials published in the Journal of the American College of Cardiologyreflect the views of the authors and do not necessarily represent the views of JACCor the American College of Cardiology.