Efficacy and Safety of Fasudil in Patients With Stable Angina: A Double-Blind, Placebo-Controlled, Phase 2 Trial
Clinical Trial
Objectives:
This study sought to evaluate the efficacy and safety of fasudil, an orally available rho kinase inhibitor, in patients with stable angina.
Background:
Several small, non–placebo-controlled trials suggest that fasudil reduces myocardial ischemia in patients with stable or vasospastic angina.
Methods:
In a multicenter, double-blind, placebo-controlled, randomized trial, the efficacy and safety of fasudil were evaluated in stable angina patients. Of the 206 patients screened, 84 patients with reproducible exercise times were randomized 1:1 to fasudil or placebo. Nitroglycerin as needed and a beta- or calcium-channel blocker were allowed. Fasudil or matching placebo was force-titrated from 20 mg three times daily to 80 mg twice daily with 20 mg twice-daily increments every two weeks. Symptom-limited exercise testing was performed after two, four, six, and eight weeks of treatment.
Results:
At peak, exercise duration was significantly improved at all visits in both groups, although exercise duration was numerically greater in patients receiving fasudil versus those receiving placebo. Time to ≥1 mm ST-segment depression was increased with fasudil at both peak and trough compared with placebo (172.1 s vs. 44.0 s, p = 0.001, and 92.8 s vs. 26.4 s, p = 0.02, respectively). Fasudil improved Seattle Angina Questionnaire scores. No significant differences in Canadian Cardiovascular Society class, time to angina, or frequency of angina or nitroglycerin use were noted between groups. Fasudil did not affect heart rate or blood pressure, and was well tolerated.
Conclusions:
Fasudil up to 80 mg three times daily significantly increased the ischemic threshold of angina patients during exercise with a trend toward increased exercise duration. Further investigation of fasudil doses >80 mg three times daily is indicated.
Introduction
Chronic stable angina, stimulated by emotional or physical stress, is the initial symptom in about 50% of patients with ischemic heart disease (1). Current treatment options include lifestyle management, pharmacotherapy to reduce myocardial oxygen demand and/or to increase myocardial blood flow, surgical or percutaneous revascularization procedures, and several alternative procedures, including transmyocardial revascularization and enhanced external counterpulsation (1–3). However, many patients remain symptomatic while receiving drug therapy or despite revascularization procedures. Thus, additional therapeutic options are needed.
Rho kinase, an intracellular signaling molecule involved in the vascular smooth muscle contractile response to agonists such as acetylcholine, angiotensin II, endothelin, norepinephrine, platelet-derived growth factor, and serotonin (4–6), has been proposed as a therapeutic target for treating stable angina. In smooth muscle cells, contraction is stimulated by G-protein–coupled receptors, which activate Rho, which subsequently activates Rho kinase (7). Rho kinase phosphorylates and inactivates myosin regulatory light chain (MRLC) phosphatase. In the absence of a functional MRLC phosphatase, MRLC remains in the active (phosphorylated) form, and interaction between actin and myosin results in sustained contraction. Animal models of coronary artery spasm have shown that Rho kinase inhibitors effectively suppress vasoconstriction (8,9). Similar results have been obtained during in vivo studies of human arteries (10).
An intravenous formulation of fasudil, a selective Rho kinase inhibitor (11), is approved in Japan to prevent cerebral vasospasm after subarachnoid hemorrhage (12) and has been considered for treatment of angina. Several phase 1 studies were conducted in patients with vasospastic angina (either angiographically detectable or microvascular) who developed electrocardiographic evidence of ischemia in response to acetylcholine. The results showed that acetylcholine-stimulated ischemia was prevented in ≥85% of patients by a 15-min intracoronary infusion of 4.5 mg fasudil (13,14).
Fasudil is bioavailable after oral administration (15) and has a half-life of 5.5 ± 0.87 h in tablet form (16). In phase 2 dose-finding trials conducted in Japanese patients with stable effort angina, fasudil monotherapy at doses ranging from 5 mg three times daily to 40 mg three times daily increased maximum exercise time and time to the onset of ≥1 mm ST-segment depression compared with baseline. Fasudil was well tolerated, with minimal effects on blood pressure or heart rate at rest or during exercise (15). However, these trials were not placebo-controlled, and use of concomitant cardiovascular drugs was not reported. Furthermore, the Japanese patient population studied has an increased tendency toward vasospasm (15).
This phase 2, placebo-controlled, dose-escalation study was designed to evaluate the efficacy and safety of fasudil at doses up to 80 mg three times daily in American patients with stable angina already receiving standard medical therapy for cardiovascular disease.
Methods
Patients
Patients
Male and female patients (ages 30 to 80 years) with evidence of coronary artery disease and stable angina (Canadian Cardiovascular Society [CCS] grading [17] class 2 or 3) for at least eight weeks were enrolled in the study. Patients with unstable angina or with angina of CCS class 1 or 4 were excluded from the study. Patients able to exercise for <3 min or for >10 min in the qualifying exercise treadmill testing (ETT) during the run-in period (>12 min in the final qualifying ETT) or with variability in exercise time of more than ±15% were also excluded. Additional exclusion criteria included patients with untreated life-threatening ventricular arrhythmias, those with underlying disease other than coronary artery disease resulting in a life expectancy of <12 months, patients with a myocardial infarction or those undergoing coronary artery bypass surgery in the previous 3 months, patients with angioplasty in the previous 6 (without stent) or 12 (with stent) months, and patients who received transmyocardial laser revascularization within the previous 3 months or enhanced external counterpulsation in the previous 12 months.
Study design
This was a multicenter, double-blind, placebo-controlled, forced-titration, parallel group study, comprising a three-week run-in period and an eight-week double-blind treatment period. During treatment, patients were randomized to receive either fasudil (20 mg three times daily, escalating in 20-mg increments at two-week intervals to 80 mg three times daily) or matching placebo in a 1:1 ratio (Fig. 1).

Schematic diagram of the study design. Exercise testing (X) was performed before dosing (trough), 1 h after dosing (peak), and 4 h after dosing of both fasudil and matching placebo tablets. tid = three times daily.
Efficacy end points
The primary efficacy end point was the change from baseline in total ETT duration at peak after two, four, six, and eight weeks of treatment. Secondary efficacy end points were changes from baseline in total ETT duration at trough and at four hours after dosing and the change from baseline in time to ≥1-mm ST-segment depression at peak after two, four, six, and eight weeks of treatment.
Tertiary efficacy end points were assessed after two, four, six, and eight weeks of treatment as well. These included changes from baseline in time to ≥1-mm ST-segment depression at trough and four hours after dosing, time of onset of angina, ≥1 class reduction in CCS angina class, angina attack frequency, weekly sublingual nitroglycerin consumption, and scales of the Seattle Angina Questionnaire (SAQ) (18).
Safety end points
All safety variables (adverse events, laboratory abnormalities, vital signs, and electrocardiogram [ECG]) were assessed at baseline and at subsequent visits. Additional visits at weeks 5 and 7 were scheduled for evaluation of safety data when laboratory test data and any significant adverse events were assessed. A central laboratory (Covance Laboratories Inc., Indianapolis, Indiana) analyzed clinical laboratory samples.
Experimental phases
Run-in period
Run-in period
During the run-in period, long-acting nitrates were discontinued, and patients underwent a one-week washout of anti-anginal drugs excluding sub-lingual nitroglycerin and one anti-anginal medication (beta-blocker or calcium-channel blocker). This was followed by a two-week single-blind, placebo run-in period to obtain baseline ETT data.
During the single-blind run-in phase, patients performed up to three qualifying ETTs according to a modified Balke protocol (Appendix), showing exercise-induced ST-segment depression ≥1 mm compared with baseline associated with grade 3 or 4 angina. The first ETT was to show an ability to exercise for at least 3 min but no more than 10 min before stopping because of angina of moderate severity (grade 3 or 4 angina). A subsequent ETT was performed within three to five days of the first, with the difference in exercise duration expected to decrease within ±15% of the first ETT. In patients not achieving this target, a third ETT could be performed. Patients achieving a difference in exercise duration within ±15% of the second ETT with exercise duration <12 min were included in the study. In addition, an ST-segment depression of ≥1 mm associated with grade 3 or 4 angina was required in each ETT. Patients who qualified for inclusion in the study received one dose of single-blind placebo medication, and symptom-limited exercise tests were repeated at one and four hours after dosing. The ETT data were obtained at each time point and, together with the last qualifying ETT, were used as the baseline ETTs.
Treatment period
The run-in period was followed by an eight-week double-blind period with administration of increasing doses of fasudil or placebo (Fig. 1). During the double-blind treatment phase, ETT was repeated before (trough) and 1 h (peak) and 4 h after dosing at day 1, and after 2, 4, 6, and 8 weeks of treatment. A 12-lead ECG and vital sign measurements in both supine and standing positions were taken before each ETT at baseline and after two, four, six, and eight weeks of treatment. An ECG was recorded every 30 s during exercise, and blood pressure was recorded during the final 30 s of exercise. The ST-segment depressions were measured manually. All rest and exercise ECG data were analyzed by the St. Louis University Core Laboratory, St. Louis, Missouri.
Ethical considerations
An independent ethics committee, institutional review board, or research ethics board approved the study protocol at each of the 33 participating study centers. All protocol amendments were subjected to the same approval process. The study was conducted in accordance with the ethical principles laid out in the Declaration of Helsinki, the Food and Drug Administration Code of Federal Regulations, and the International Conference of Harmonization–Good Clinical Practice guidelines. All patients gave written informed consent to their participation in the study.
Statistical analysis
Based on an expected detectable difference of 45 sec (0.75 min) between treatment and placebo groups in change from baseline in peak exercise duration, the sample size was estimated at 40 patients per treatment group. This provided an 85% statistical power to detect the difference, at the alpha = 0.05 significance level, based on a two-tailed ttest with an assumed standard deviation of 1.1 min.
One-way analysis of variance (equivalent to a ttest when two groups are compared) was used to analyze the primary, secondary, and tertiary efficacy variables in the efficacy-evaluable set. The exceptions to this were time to ≥1 mm ST-segment depression (log rank test) and change in CCS angina class (Fisher exact test).
Results
Patients’ baseline characteristics
Patients’ baseline characteristics
A total of 206 patients were screened for entry into the study. Of these, 122 patients were excluded, primarily because of failure to meet entry criteria (Fig. 2).The 84 patients randomized to treatment (41 in the fasudil group and 43 in the placebo group) all received at least one dose of study medication. There were no statistical differences in baseline characteristics in the two treatment groups (Table 1).Patients entered into the study were receiving a stable dose of one antianginal medication (Table 2).The majority (65%) received beta-blockers during the double-blind phase, whereas 54% used short-acting nitrates for the relief of acute anginal attacks.

Patient disposition during the study.
| Variable | Placebo (n = 43) | Fasudil (n = 41) | p Value⁎ |
|---|---|---|---|
| Age (yrs) | 0.435 | ||
| Mean (SD) | 64.4(9.62) | 66.0(9.42) | |
| Min-max | 49–80 | 44–82 | |
| <65, n(%) | 21(49) | 18(44) | 0.668 |
| Gender | 1.000 | ||
| Male, n (%) | 32(74) | 31(76) | |
| CCS angina class | 0.738 | ||
| 2, n (%) | 3(91) | 37(90) | |
| 3, n (%) | 4(9) | 4(10) | |
| Weekly number of anginal attacks | 0.167 | ||
| n | 38 | 39 | |
| Mean (SD) | 2.4(3.84) | 4.3(7.37) | |
| Min-max | 0–16 | 0–34 | |
| Weekly nitroglycerin tablet use | 0.115 | ||
| n | 38 | 39 | |
| Mean (SD) | 0.5(1.67) | 2.2(6.26) | |
| Min-max | 0–10 | 0–33 | |
| Exercise duration at peak | 0.374 | ||
| n | 43 | 41 | |
| Mean (SD) | 443.7(144.20) | 470.0(123.17) | |
| Min-max | 176–690 | 228–690 | |
| Time to ≥1 mm ST-segment depression at peak (s) | 0.107 | ||
| n | 34 | 36 | |
| Mean (SD) | 333.1(116.39) | 382.4(142.81) | |
| Min-max | 150–540 | 90–660 | |
| Disease perception/quality of life score† | 0.364 | ||
| n | 42 | 40 | |
| Mean (SD) | 66.3(19.65) | 63.0(24.26) | |
| Min-max | 25–100 | 8–100 | |
| Heart rate (beats/min) | NS | ||
| n | 39 | 39 | |
| Resting supine, mean (SD) | 68.4(14.34) | 67.9(12.03) | |
| Peak exercise, mean (SD) | 114.1(18.56) | 118.2(17.86) | |
| Systolic blood pressure (mm Hg) | NS | ||
| n | 39 | 39 | |
| Resting supine, mean (SD) | 137.5(22.59) | 137.5(15.48) | |
| Peak exercise, mean (SD) | 171.8(22.94) | 167.8(19.73) | |
| Diastolic blood pressure (mm Hg) | NS | ||
| n | 39 | 39 | |
| Resting supine, mean (SD) | 79.9(9.34) | 79.3(8.61) | |
| At peak exercise, mean (SD) | 84.4(14.57) | 85.0(13.83) |
| Concomitant Medication | Placebo (n = 43) | Fasudil (n = 41) |
|---|---|---|
| Nitrates | 20(47) | 25(61) |
| Beta-blockers | 30(70) | 25(61) |
| Calcium channel blockers | 9(21) | 8(20) |
| ACE inhibitors | 16(37) | 14(34) |
| Angiotensin receptor blockers | 7(16) | 8(20) |
| Diuretics | 11(26) | 12(29) |
| HMG-CoA inhibitors | 32(74) | 28(68) |
| Antiplatelet agents | 35(81) | 35(85) |
| Drugs for diabetes | 7(16) | 5(12) |
All patients who received at least one dose of study medication and had a follow-up evaluation were included in the efficacy analysis set. All 84 patients randomized to treatment were included in this data set. A total of nine patients (five in the fasudil group, four in the placebo group) discontinued the study prematurely, primarily because of adverse events (Fig. 2).
Efficacy end points
Primary efficacy variable: Treadmill exercise duration at peak
Primary efficacy variable: Treadmill exercise duration at peak
At peak, the change in ETT duration compared with baseline was significantly improved at all visits in both the fasudil and placebo groups. There was a numerically greater but not statistically significant increase in ETT duration at peak in patients receiving fasudil compared with those receiving placebo after two, four, six, and eight weeks of treatment (Fig. 3).At eight weeks (80 mg three times daily), the increase in time to exercise cessation was 118.4 ± 131.6 s in patients given fasudil compared with 86.1 ± 142.2 s in patients given placebo (p = 0.311). Improvement seemed to be dose- and/or time-dependent.

Changes in exercise treadmill testing duration from baseline at peak for fasudil- (solid bars)and placebo-treated (open bars)patients (mean ± standard deviation). tid = three times daily.
Secondary efficacy variables
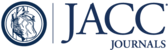
At peak, both the placebo and fasudil treatment groups showed significant within-group improvements from baseline in the mean time to ≥1 mm ST-segment depression. In the fasudil group, significant improvements were seen at all visits (week 2, p = 0.005; weeks 4, 6, and 8, p < 0.001), whereas in the placebo group, significant improvements were observed at weeks 2, 4, and 6 (p = 0.027, 0.007, and 0.004, respectively). The mean change from baseline in time to ≥1 mm ST-segment depression (myocardial ischemia) at peak was greater in the fasudil-treated group compared with the placebo group at weeks 2, 4, 6, and 8 (Fig. 4).This difference reached statistical significance at eight weeks (80 mg three times daily), when the time to myocardial ischemia was 172.1 ± 124.5 s for patients given fasudil compared with 44.0 ± 109.6 s in the placebo group (p < 0.001).

Changes in mean time to ≥1 mm ST-segment depression from baseline for fasudil- (solid bars)and placebo-treated (open bars)patients. *p = 0.001. tid = three times daily.
There were no consistent numerical differences in ETT duration, either at trough or at four hours after dosing, between fasudil and placebo after two, four, six, or eight weeks of treatment.
Tertiary end points
At trough, the mean time to ≥1 mm ST-segment depression was significantly increased to 92.8 s with 80-mg three-times-daily fasudil (week eight) versus 26.4 s with placebo treatment (p = 0.02). There was also a statistically significant treatment effect for time to ≥1 mm ST-segment depression (p = 0.006) as assessed by the log-rank test. However, no significant differences between treatment groups were observed at four hours after dosing.
Fasudil had little effect on several additional parameters of efficacy. No significant changes in the time to onset of angina, weekly frequency of angina, or use of nitroglycerin were noted. A dose- and time-related trend in the percentage of patients with ≥1 CCS class improvement was observed, although the differences between the placebo and fasudil groups did not reach significance (Fig. 5).

Improvements in angina by ≥1 Canadian Cardiovascular Society angina class in patients treated with fasudil (solid bars)and placebo (open bars). tid = three times daily.
Nevertheless, fasudil improved measures of quality of life. The SAQ physical limitation scale for patients receiving fasudil was improved at all visits, whereas the scores for placebo patients worsened. The differences in SAQ score between patients receiving fasudil and those receiving placebo were significant at the 60- and 80-mg three-times daily fasudil doses (Fig. 6A).The SAQ treatment satisfaction scores (Fig. 6B) also improved with fasudil treatment, with a statistically significant difference between patients receiving fasudil and those receiving placebo observed at the 40- and 60-mg three-times-daily doses.

Improvement in Seattle Angina Questionnaire score. (A)Physical limitation scale. (B)Treatment satisfaction scale. *p < 0.05. tid = three times daily. Open bars= placebo; solid bars= fasudil.
Safety
Fasudil was well tolerated at a dose of 20 to 80 mg three times daily. A total of 49 patients (58%) reported adverse events during the double-blind treatment period. The incidence of adverse events was similar in the two treatment groups, with 23 of 43 patients (53%) in the placebo group and 26 of 41 patients (63%) in the fasudil group reporting adverse events. Because only one or two patients experienced any given syndrome and none of the differences were statistically significant, these disorders are described by organ system. The body systems apparently more frequently affected in the fasudil group than in the placebo group included the skin and subcutaneous tissue, and the vascular system (Table 3).Skin disorders in patients treated with fasudil were heterogeneous, including allergic dermatitis, a bruise, diaphoresis, facial erythema, erythropapular rash, erythematous rash, hives, and keratosis. Similarly, vascular disorders in patients receiving fasudil were heterogeneous, including facial flushing, ecchymoses, hypotension, hypertension, and a Raynaud-like phenomenon.
| Body System | Placebo (n = 43) n (%) Specific Events, No. of Patients | Fasudil (n = 41) n (%) Specific Events, No. of Patients |
|---|---|---|
| Skin and subcutaneous disorders |
|
|
| Nervous system disorders |
|
|
| Vascular disorders |
|
|
| Infections and infestations |
|
|
| Cardiac disorders |
|
|
The majority of the adverse events reported were classified as mild to moderate. There were no deaths during the study. Two patients (5%) in the placebo group and five patients (12%) in the fasudil group reported severe adverse events. In the placebo group, the severe events were myocardial infarction, unstable angina, and upper gastrointestinal hemorrhage. In the fasudil group, the severe events were worsened chronic stable angina pectoris, chest pain, increased ocular pressure, headache, hives, and hypertension.
The proportion of patients with adverse events considered to be related to study medication in the opinion of the investigator was higher in the placebo group (30% [13 of 43] vs. 22% [9 of 41] in the fasudil group).
No dose- or time-dependent trends in adverse events were observed between the 20- and 60-mg three-times-daily fasudil groups. At these doses, no difference in the incidence of adverse events between fasudil and placebo groups was observed. Although slightly more patients reported adverse events at the 80-mg three-times-daily fasudil dose, there was no significant difference compared with the placebo group.
Within-group changes from baseline were observed for some laboratory parameters. Both aspartate transferase and alanine transferase were decreased in both treatment groups, and platelet count was decreased in the placebo group and increased in the fasudil group but with no significant difference between treatment groups. A statistically significant but not clinically significant increase in serum creatinine was observed in the fasudil group (from 1.02 to 1.08 mg/dl, p < 0.05) but not in the placebo group (1.03 to 1.01 mg/dl, p < 0.05). The mean changes from baseline for the other laboratory parameters were minimal, with no observable within-group or between-group trends.
There were few statistically significant differences between the effects of fasudil and placebo on heart rate, blood pressure, or the product of heart rate and systolic blood pressure at any time point, and there was no evidence of either treatment-related or dose-dependent effects during exercise at peak (Table 4).Similarly, few changes in 12-lead ECG findings were noted during the study. No change in QT or QTc Fridericia from baseline were found at any time after dosing.
| Parameter | Placebo (n = 36) | Fasudil (n = 33) |
|---|---|---|
| Heart rate (beats/min) | 1.8±13.13 | 1.2±14.77 |
| Systolic blood pressure (mm Hg) | −5±20.23 | −0.1±19.46 |
| Diastolic blood pressure (mm Hg) | −1.2±7.71 | −3.1±9.55 |
| Double product (systolic blood pressure·heart rate or mm Hg·beats/min) | −263±3,569 | 253±3,727 |
Discussion
This phase 2 dose-finding trial in patients with stable angina showed that titrating fasudil to 80 mg three times daily over eight weeks improved exercise time compared with baseline, with a statistical trend toward improvement compared with placebo. A significant, nearly four-fold increase in mean time to ≥1 mm ST-segment depression (myocardial ischemia) compared with placebo was observed at peak (1 h after dosing) with a fasudil dose of 80 mg three times daily. Lesser effects of fasudil on myocardial ischemia were observed four hours after dosing and at trough. Administration of fasudil was associated with significant improvements in SAQ physical limitation and treatment satisfaction scores compared with placebo. A favorable trend in CCS class was also shown. No differences in time to onset of angina, weekly frequency of angina, or use of nitroglycerin were noted between the treatment groups. The rates of adverse events and withdrawal because of adverse events were similar in both treatment groups. Most adverse events were mild and not considered related to study medication.
Although the primary end point was not achieved, the results obtained in this study are promising. In retrospect, the study was underpowered to detect an increase in exercise time with fasudil therapy. In the power calculation, the magnitude of the anticipated effect was overestimated (0.75 min vs. an actual difference of 0.5 min) and the standard deviation of patient exercise times was underestimated (1.1 min vs. 1.98 min in the fasudil group and 2.37 min in the placebo group). Thus, a larger study (approximately 300 per group) is required to determine whether fasudil therapy is associated with improved exercise time.
However, the study was appropriately powered to detect differences in time to ≥1 mm ST-segment depression, the secondary end point. This measurement is more reproducible than exercise testing, and changes in this parameter are placebo-independent and associated with a poor prognosis (19). Furthermore, the magnitude of the effects of fasudil on ≥1 mm ST-segment elevation are comparable to the magnitude of changes observed in separate studies of the beta-blocker propranolol and nine calcium-channel blockers compared with placebo (20). These established therapies for angina increased the time to myocardial ischemia by 1.4 to 2.7 min (20). The 2.1-min improvement observed with fasudil is within this range and was achieved despite concomitant use of background medication. In contrast, ranolazine, a partial fatty acid oxidation inhibitor in development for stable angina, increased the time to myocardial ischemia at peak compared with placebo by 55.6 ± 8.2 s (mean ± standard error) as monotherapy (1,000 mg twice daily) and by 34.5 ± 11.9 s when given in addition to atenolol, amlodipine, or diltiazem (21,22).
The results of this study seem to differ from the results of the previous phase 2 trials with fasudil (15). For example, more end points improved significantly in the previous trials, including maximum exercise time, the number of angina attacks per week and use of sublingual nitroglycerin. However, these studies were not placebo-controlled. Significance in the previous study was compared with baseline, whereas significance in this trial was determined compared with placebo. When the results of this trial are compared with baseline, maximum exercise time, the frequencies of angina attacks, and nitroglycerin use significantly increased in both the placebo and fasudil treatment groups. Thus, these results are similar to those of the previous study and emphasize the importance of comparison of active therapy to a placebo.
Other differences in the results between this and previous trials may be meaningful. Whereas no dose-response relationship in time to myocardial ischemia was observed with fasudil doses of 5 mg three times daily to 40 mg three times daily (15), an apparent dose-dependent trend was observed in this trial with doses ranging from 20 mg three times daily to 80 mg three times daily. The magnitude of the increase in time to ≥1 mm ST-segment depression at 80 mg three times daily in this study was 172 s (2.87 min), compared with 109 s (1.8 min) at 40 mg three times daily (this study) and 78 s (1.3 min) at 40 mg three times daily (previous trial) (15).
Both in the current study and in previous trials, fasudil was well tolerated at the doses tested. No deaths occurred during these studies, and few serious treatment-related adverse events were observed. Transient headache was the most frequent adverse event in both the fasudil and placebo groups (15); however, skin and vascular disorders seemed to differ most between the groups. The contribution of fasudil-mediated vasodilation to these adverse events should be explored. However, no clinically important changes in laboratory results were found, and no adverse effects on heart rate, blood pressure, or ECG were reported.
Taken together, these data suggest that the optimum oral dose of fasudil for patients with stable angina may be >80 mg three times daily. No plateau in the dose-response relationship with regard to an increase in exercise time or changes in ST-segment depression was observed for fasudil doses up to 80 mg three times daily. Furthermore, the significant decrease in myocardial ischemia found at peak after administration of fasudil may be better maintained between doses with a higher starting dose. Suboptimal dosing may also explain the lack of a significant effect on exercise time and the lack of reduction in anginal frequency and nitroglycerin use. Because fasudil is well-tolerated by patients at the doses tested to date, evaluation of higher dosing seems to be feasible and warranted.
Because study duration and dose are linked in this study, increased study duration may influence the results, particularly with respect to the frequency of anginal episodes and weekly nitroglycerin use. It is encouraging that quality of life improvements were observed within the study period. A future study should examine the effects of higher doses of fasudil for a longer period of time.
Because of its unique mechanism of action, fasudil may be a useful adjunctive therapy to standard therapies for stable angina. By inhibiting Rho kinase, which mediates the vasoconstriction stimulated by a wide variety of agonists, fasudil may inhibit the effects of vasoconstrictors that are unaffected by current therapies. Although it is likely that the optimal dose of fasudil for treatment of stable angina has not yet been established, the current efficacy and safety results justify further investigation of its therapeutic properties.
Appendix
For the modified Balke protocol as well as a list of the participating investigators in the Fasudil Study Group, please see the online version of this article.
1. : "ACC/AHA/ACP-ASIM guidelines for the management of patients with chronic stable angina: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines". J Am Coll Cardiol 1999; 33: 2092.
2. :
Update: measuring antianginal drug efficacy using exercise testing for chronic angina. Improved exercise performance with a new class of drugs, the pFOX inhibitors . In: Hurst’s the Heart . Edited by . Columbus, OH: McGraw-Hill2004: 1032.3. : "Current medical management of chronic stable angina". J Cardiovasc Pharmacol Ther 2004; 9: S11. quiz S98–9.
4. : "Dedicated myosin light chain kinases with diverse cellular functions". J Biol Chem 2001; 276: 4527.
5. : "Rho-kinase as a novel therapeutic target in treatment of cardiovascular diseases". J Cardiovasc Pharmacol 2002; 39: 319.
6. : "Rho kinase inhibitors as potential therapeutic agents for cardiovascular diseases". Curr Opin Investig Drugs 2003; 4: 1065.
7. : "Rho GTPases in cell biology". Nature 2002; 420: 629.
8. : "Inhibition of myosin phosphatase by upregulated rho-kinase plays a key role for coronary artery spasm in a porcine model with interleukin-1beta". Circulation 2000; 101: 1319.
9. : "Rho-kinase-mediated pathway induces enhanced myosin light chain phosphorylations in a swine model of coronary artery spasm". Cardiovasc Res 1999; 43: 1029.
10. : "Involvement of rho-kinase in agonists-induced contractions of arteriosclerotic human arteries". Arterioscler Thromb Vasc Biol 2002; 22: 243.
11. : "Agonist-induced regulation of myosin phosphatase activity in human platelets through activation of Rho-kinase". Blood 1999; 93: 3408.
12. : "Effect of AT877 on cerebral vasospasm after aneurysmal subarachnoid hemorrhage. Results of a prospective placebo-controlled double-blind trial". J Neurosurg 1992; 76: 571.
13. : "Suppression of coronary artery spasm by the Rho-kinase inhibitor fasudil in patients with vasospastic angina". Circulation 2002; 105: 1545.
14. : "Rho-kinase inhibition with intracoronary fasudil prevents myocardial ischemia in patients with coronary microvascular spasm". J Am Coll Cardiol 2003; 41: 15.
15. : "Anti-anginal effect of fasudil, a Rho-kinase inhibitor, in patients with stable effort angina: a multicenter study". J Cardiovasc Pharmacol 2002; 40: 751.
16. : "Assessment of absorption of rho kinase inhibitor fasudil at different sites of the human gastrointestinal tract". (abstr) Clin Pharmacol Ther 2004; 75: P6.
17. : "Grading of angina pectoris". Circulation 1976; 54: 522.
18. : "Monitoring the quality of life in patients with coronary artery disease". Am J Cardiol 1994; 74: 1240.
19. : "Prognostic value of the admission electrocardiogram in acute coronary syndromes". JAMA 1999; 281: 707.
20. : "A comparison of nine calcium ion antagonists and propranolol: exercise tolerance, heart rate and ST-segment changes in patients with chronic stable angina pectoris". Eur J Clin Pharmacol 1987; 32: 539.
21. : "Effects of ranolazine with atenolol, amlodipine, or diltiazem on exercise tolerance and angina frequency in patients with severe chronic angina: a randomized controlled trial". JAMA 2004; 291: 309.
22. : "Anti-ischemic effects and long-term survival during ranolazine monotherapy in patients with chronic severe angina". J Am Coll Cardiol 2004; 43: 1375.
Abbreviations and Acronyms
| CCS | Canadian Cardiovascular Society |
| ECG | electrocardiogram |
| ETT | exercise treadmill testing |
| MRLC | myosin regulatory light chain |
| SAQ | Seattle Angina Questionnaire |
Footnotes
Supported by Berlex Laboratories Inc. Drs. Keefe and Morales-Ballejo are employees of and own stock in Berlex Laboratories Inc. Drs. Vicari, Chaitman, Smith, Chrysant, Tonkon, Weiss, and Bittar have received research grants from Berlex Laboratories Inc.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}