Acute Lead Dislodgements and In-Hospital Mortality in Patients Enrolled in the National Cardiovascular Data Registry Implantable Cardioverter Defibrillator Registry
Heart Rhythm Disorders
Objectives:
We sought to describe the incidence of acute lead dislodgements and the consequences of these events in patients enrolled in the National Cardiovascular Data Registry (NCDR) Implantable Cardioverter-Defibrillator (ICD) Registry.
Background:
Lead dislodgements are common adverse events in patients undergoing ICD implants. Little is known regarding who is at risk and the consequences of these events.
Methods:
Patients enrolled between April 2006 and September 2008 were included. Acute lead dislodgement was defined as movement of the lead requiring another procedure for repositioning before discharge.
Results:
Acute dislodgement occurred in 2,628 of 226,764 patients. Univariate variables associated with dislodgements included older age, female sex, and patients with atrial fibrillation, chronic lung disease, cerebrovascular disease, nonischemic cardiomyopathy, and lower ejection fractions (all p < 0.002). After multivariate adjustment, factors associated with an increased risk for dislodgement included New York Heart Association functional class IV heart failure, atrial fibrillation/flutter, having a cardiac resynchronization therapy-defibrillator device, and procedures performed by physicians trained under alternative pathways. A teaching/training hospital setting was not a factor (p = 0.64). Acute dislodgements had increased odds for other adverse events including cardiac arrest, cardiac tamponade, device infection, pneumothorax, and in-hospital death even after adjustment for potential confounders (all p < 0.0001).
Conclusions:
Acute lead dislodgements occur more often in patients with more comorbidities and in patients undergoing implants by nonelectrophysiology-trained implanters. These events were strongly associated with increased odds for in-hospital death.
Introduction
Lead dislodgements are common complications (1,2), often resulting in prolonged hospital stays and increased costs (3). While the frequency of long-term lead dislodgements ranges between 1.8% and 8% (4–8), little is known about the frequency of acute lead dislodgements and risk factors associated with these events. Utilizing the National Cardiovascular Data Registry (NCDR) Implantable Cardioverter-Defibrillator (ICD) Registry, we sought to determine the prevalence of acute lead dislodgements, factors associated with these complications, and the prevalence of other more serious adverse events caused by or closely associated with them.
Methods
Data source and study cohort
Data source and study cohort
Analyses used data from the NCDR ICD Registry. All procedures performed between April 2006 and September 2008 were screened; patients with prior ICDs were excluded.
Outcomes
The occurrence of an acute lead dislodgement was the primary end point, and the occurrence of other adverse events caused by or closely associated with the dislodgement was the secondary end point. Acute dislodgements were defined as those involving movement of the lead requiring another procedure for repositioning before patient discharge. To account for potential variations in data coding, patients who experienced cardiac perforations were also included as having experienced an acute lead dislodgement. Other adverse events included cardiac arrest, drug reaction, coronary venous dissection, hematoma, pneumothorax, peripheral embolus, superficial phlebitis, myocardial infarction, pericardial tamponade, infection related to device, and in-hospital death.
Independent confounders
Confounding variables considered included admission characteristics, patient comorbidities, and physician/hospital characteristics. The rate of missing data was extremely low for all variables (<0.5%) with the exception of ejection fraction (1.5%). To avoid case-wise deletion, missing values were imputed. For categorical variables, the missing variables were imputed with the most common value present in the cohort. For continuous variables, the missing values were imputed as the median among those with the data present. In cases of missing data, dummy variables were constructed to indicate where the variable was missing. In multivariable models, both imputed values and dummy variables were included.
Statistical methods
Baseline demographic and clinical factors were compared between patients with acute dislodgements and patients without using chi-square testing and ttests as appropriate. Independent associations of various characteristics were identified using a hierarchical logistic regression model to account for clustering of patients within hospitals and regional differences in demographics. Variables selected for the multivariate analyses were chosen based on the plausibility that they could be associated with the end point. The analyses were then repeated for subjects undergoing cardiac resynchronization therapy-defibrillator (CRT-D) implantation. Finally, associations of acute dislodgements with other adverse events were identified. Significant variables were those with a p < 0.05. All analyses were approved by the Yale Human Investigation Committee and performed using the SAS Statistical Package version 9.1 (SAS Institute, Cary, North Carolina).
Results
Baseline demographics and characteristics associated with lead dislodgements
Baseline demographics and characteristics associated with lead dislodgements
During the period studied, 296,534 implants were recorded in the ICD Registry. After excluding patients with previous ICDs, 226,764 remained. Among 226,764 entries, 79,909 (35.2%) underwent CRT-D implantation. Baseline demographics of the entire cohort are illustrated in Table 1.Acute dislodgement was the most common adverse event reported, and occurred in 2,628 (1.2%) patients. For the 3 types of device systems, namely, single-chamber, dual-chamber, and CRT-D, the rates were 0.56%, 0.97%, and 1.78%, respectively. Unadjusted variables associated with acute dislodgements included older age, female sex, more advanced heart failure, and a greater number of comorbidities (Table 2).Patients who had pre-existing pacemaker leads or those undergoing CRT-D devices were also more likely to have experienced an acute dislodgement. In fact, 54.3% of dislodgements were in patients who had undergone CRT-D implants.
| Age, yrs | 67.5±13.0 |
| Female | 27.0% |
| Race | |
| White | 78.8% |
| Black | 12.8% |
| Hispanic | 5.4% |
| Other | 3.1% |
| NYHA functional class | |
| I | 12.3% |
| II | 35.7% |
| III | 47.6% |
| IV | 4.4% |
| Atrial fibrillation/flutter | 31.3% |
| Cardiac transplantation | 0.2% |
| Nonischemic cardiomyopathy | 32.1% |
| Prior coronary bypass | 34.0% |
| Prior pacemaker implanted | 11.2% |
| History of CVA | 14.5% |
| Chronic lung disease | 22.8% |
| Diabetes mellitus | 37.2% |
| Hypertension | 75.2% |
| GFR ≥60 ml/min | 58.7% |
| Hemodialysis | 4.2% |
| Left ventricular ejection fraction, % | 27.5±10.7 |
| QRS duration, ms | 125.4±34.3 |
| Left bundle branch block | 26.0% |
| Single-chamber ICD | 24.0% |
| Dual-chamber ICD | 40.6% |
| CRT-D | 35.2% |
| Variable | Acute Dislodgement | No Acute Dislodgement | p Value |
|---|---|---|---|
| Age, yrs | 68.6±12.7 | 67.5±13.0 | <0.0001 |
| Female | 31.9% | 27.0% | <0.0001 |
| Race | 0.005 | ||
| White | 81.5% | 78.7% | |
| Black | 11.5% | 12.8% | |
| Hispanic | 3.8% | 5.4% | |
| Other | 3.2% | 3.1% | |
| NYHA functional class | <0.0001 | ||
| I | 9.0% | 12.4% | |
| II | 26.4% | 35.8% | |
| III | 58.4% | 47.4% | |
| IV | 6.2% | 4.4% | |
| Atrial fibrillation | 35.3% | 31.3% | <0.0001 |
| Cardiac transplantation | 0.2% | 0.2% | 0.4755 |
| Ischemic cardiomyopathy | 61.8% | 68.0% | <0.0001 |
| Prior pacemaker | 14.0% | 11.2% | <0.0001 |
| CVA | 16.5% | 14.5% | 0.0035 |
| Lung disease | 25.8% | 22.8% | 0.0002 |
| Diabetes mellitus | 37.7% | 37.1% | 0.5282 |
| Hypertension | 74.2% | 75.2% | 0.2321 |
| GFR ≥60 ml/min | 57.8% | 58.7% | 0.3349 |
| Ejection fraction, % | 26.8±10.4 | 27.5±10.7 | 0.0017 |
| QRS duration, ms | 134.8±35.0 | 125.3±34.3 | <0.0001 |
| Left bundle branch block | 35.0% | 25.9% | <0.0001 |
| ICD type | <0.0001 | ||
| Single-chamber | 11.6% | 24.2% | |
| Dual-chamber | 34.0% | 40.6% | |
| CRT-D | 54.3% | 35.0% | |
| LV lead implanted | <0.0001 | ||
| Coronary sinus | 49.2% | 33.2% | |
| Noncoronary sinus | 4.1% | 1.3% |
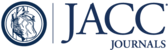
Among physician and hospital characteristics, several factors were associated with acute dislodgements and included physician's experience (as defined by volume) and training (Table 3).When physician implant volumes were broken down by quartiles (Fig. 1)and stratified by type of device implanted, acute dislodgement rates were lower for those with higher volumes, as previously reported (10), except in the case of single-chamber devices (single-chamber, p = 0.30; dual-chamber, p = 0.005; CRT-D, p = 0.002). In terms of physician training, board certification and board eligibility in electrophysiology (EP) were the only 2 factors associated with a lower likelihood of acute dislodgements. Fulfilling criteria established as an alternative training pathway (11) was not associated with fewer dislodgements. Although hospital size (i.e., bed number) had no significant effect, there appeared to be more lead dislodgements occurring in community-based institutions. The teaching status of the hospital (where trainees may be involved in these procedures) was not associated with increased risk for dislodgement.
| Variable | Acute Dislodgements | No Acute Dislodgments | p Value |
|---|---|---|---|
| Hospital type | 0.027 | ||
| Government | 1.7% | 1.5% | |
| Private/community | 86.6% | 85.1% | |
| University | 11.6% | 13.4% | |
| Teaching hospital | 55.2% | 54.7% | 0.638 |
| Physician implant volume | 135±96 | 144±101 | <0.0001 |
| Physician training | 0.011 | ||
| Board-certified EP | 75.4% | 76.3% | |
| Board-eligible EP | 5.4% | 6.0% | |
| HRS guidelines | 11.2% | 9.7% | |
| Surgery boards | 2.6% | 2.0% |

Acute Lead Dislodgements and Physician Implant Volume
Physician implant volumes were divided into quartiles (Q). Q1 represents physicians with the lowest volume, and Q4 represents those with the highest volume.
Multivariate models were generated with variables that would plausibly be associated with acute dislodgements. This demonstrated increased odds for acute dislodgements for females, for patients who had NYHA functional class IV heart failure, atrial fibrillation/flutter, and for patients who had received dual and CRT-D devices (Table 4).Patients with a history of coronary artery bypass graft surgery had decreased odds for dislodgements. Whereas hospital volume had no effect on the odds for dislodgement, physician training did. When compared with physicians who were board certified or eligible in EP, physicians who had completed an alternative training pathway (11) were the only ones with increased odds for dislodgement.
| Variable | Odds Ratio | 95% Confidence Interval |
|---|---|---|
| Age | 1.01 | 0.99–1.02 |
| Female | 1.16 | 1.07–1.25 |
| NYHA functional class II | 0.99 | 0.86–1.14 |
| NYHA functional class III | 1.14 | 0.99–1.31 |
| NYHA functional class IV | 1.23 | 1.01–1.50 |
| Atrial fibrillation/flutter | 1.09 | 1.01–1.18 |
| Nonischemic cardiomyopathy | 1.10 | 1.01–1.19 |
| Prior coronary artery bypass | 0.82 | 0.75–0.90 |
| Prior pacemaker | 0.96 | 0.87–1.07 |
| Chronic lung disease | 1.10 | 1.01–1.19 |
| Dual-chamber ICD | 1.70 | 1.50–1.92 |
| CRT-D | 2.92 | 2.57–3.32 |
| HRS guidelines | 1.23 | 1.07–1.42 |
| Surgery boards | 1.22 | 0.95–1.56 |
| Pediatric cardiology boards | 0.93 | 0.77–1.12 |
Acute lead dislodgements in patients undergoing CRT-D implantation
Among 79,909 patients who underwent CRT-D implantation, data on the type of LV lead used was available for 99.6%. Coronary sinus leads were implanted 94.8% of the time, with noncoronary sinus leads representing 3.9%. Acute dislodgements occurred with a frequency of 1.8%. Factors associated with lead dislodgements included female sex, having nonischemic cardiomyopathy, and receiving a noncoronary sinus LV lead. Higher physician implant volumes were associated with fewer dislodgements. Electrophysiology board certification/eligibility was not a factor in this subset despite being a factor in the entire cohort. Hospital characteristics were also not significantly associated with acute dislodgements. When these variables were applied in a multivariate model, the only factor associated with dislodgement was the type of LV lead implanted. Patients receiving a noncoronary sinus lead had increased odds (odds ratio: 2.00, confidence interval: 1.65 to 2.41) for dislodgement when compared with patients receiving a coronary sinus lead. As with the entire cohort, prior coronary artery bypass grafting had decreased odds for dislodgement (odds ratio: 0.79, 95% confidence interval: 0.71 to 0.87).
Sequelae of acute lead dislodgements on length of stay and other adverse events
The average length of stay in the entire cohort was 4.7 days. Patients who had an acute dislodgement had an increased length of stay by 2.3 days. Although a majority of acute dislodgements were isolated events, 10.9% were associated with other adverse events. Table 5highlights both the minor and major events between patients with and without lead dislodgements. Minor events, including drug reactions, hematoma, and superficial phlebitis, were seen at a greater frequency among patients with dislodged leads than among patients without dislodged leads. Major complications also occurred with greater frequency among patients with lead dislodgements. These events included cardiac arrest, tamponade, pneumothorax, and device infection. After adjusting for various factors, patients with acute dislodgements had significantly greater odds for the combined major complications listed in the preceding text. More importantly, there were also greater odds for in-hospital death as a result of lead dislodgements (Table 6).
| Variable | Acute Dislodgements | No Acute Dislodgements | p Value |
|---|---|---|---|
| Length of stay | 6.9 days | 4.6 days | <0.0001 |
| Drug reaction | 0.34% | 0.09% | <0.0001 |
| Phlebitis, superficial | 0.15% | 0.04% | 0.006 |
| Hematoma | 4.15% | 0.97% | <0.0001 |
| Infection | 0.23% | 0.02% | <0.0001 |
| Peripheral embolus | 0.19% | 0.03% | <0.0001 |
| Cardiac arrest | 1.45% | 0.31% | <0.0001 |
| Cardiac perforation | 7.04% | 0.00% | <0.0001 |
| Pneumothorax | 1.56% | 0.47% | <0.0001 |
| Hemothorax | 0.42% | 0.09% | <0.0001 |
| In-hospital death | 1.29% | 0.41% | <0.0001 |
| End Point | Odds Ratio | 95% Confidence Interval | p Value |
|---|---|---|---|
| Combined events (cardiac arrest, tamponade, pneumothorax, infection) | 5.62 | 4.79–6.60 | <0.00001 |
| In-hospital death | 2.66 | 1.98–3.57 | <0.00001 |
Discussion
Patient characteristics associated with dislodgements
Patient characteristics associated with dislodgements
Acute dislodgement was the most common adverse event reported and occurred 1.2% of the time. Despite a number of unadjusted variables, only worse heart failure status and the presence of atrial fibrillation/flutter were independently associated with acute dislodgements. One could hypothesize that both of these factors contributed to more dislodged leads, perhaps because of worsening myocardial architecture and chamber size, thus compromising lead stability. A few notable “lack of associations” were also seen, including chronic lung disease (i.e., pulmonary hypertension and resultant significant tricuspid regurgitation) and a history of coronary artery bypass (i.e., lack of a right atrial appendage compromising stable atrial lead placement). Interestingly, patients who had undergone coronary bypass had a decreased risk for dislodgement. That could have been the result of surgically induced pericardial fibrosis that reduced the risk of lead perforation.
Physician training, device characteristics, and outcomes associated with dislodgements
Patients in the entire cohort who underwent implantation by physicians who had completed an EP fellowship had fewer dislodged leads. When compared with these physicians, those trained under alternative training pathways (11) were independently associated with more dislodgements. This finding did not appear to be simply a function of physician volume as the average number of implants per physician was 57.6 cases per year. What this more likely represents are inherent differences in the way the training is performed. Being trained in a formalized fellowship program where there are clear hierarchical structures of authority may encourage a freer exchange of constructive criticism, as compared with being trained where training is occurring between contemporary colleagues. With regard to hospital settings, teaching hospitals (where trainees with limited experience are involved) were not associated with a higher incidence of dislodgements.
Although the ICD registry did not record the type/location of implant of the dislodged lead, data on the type of system implanted demonstrated a graded increase in the risk for dislodgement for dual and CRT-D devices when compared with single-chamber devices. In fact, >54% of dislodgements occurred in CRT-D devices. One could hypothesize this occurring because of the LV lead; however, this may simply be a function of having more leads implanted and thus having more at risk for dislodgement.
Perhaps the most important finding from this analysis is the observation that 10.9% of acute dislodgements were associated with other adverse events. Many of these were minor, but major complications also occurred and resulted in cardiac tamponade, cardiac arrest, pneumothorax, and in-hospital death.
Study limitations
First, because of data coding issues, we incorporated cardiac perforation as a form of dislodgement. Some may argue that this is a separate entity. When we analyzed the cases excluding perforations, the findings did not change our conclusions. Second, acute dislodgements not resulting in reoperation or occurring after discharge were not included. Prior reports, however, suggest a majority of lead dislodgements tend to occur within 72 h from implant (2,12). This time period would have been covered in this analysis, as the average length of stay was >4 days. Third, this was a cross-sectional study and outcomes including other adverse events and death may have occurred after discharge (13). However, our analysis is arguably more specific and focused on the relationship of acute dislodgements with these other outcomes. Death occurring after discharge may have been secondary to other causes, and thus would be less specific in terms of its relationship to this complication. Fourth, we do not have information regarding the type/implant location of the lead that dislodged. That is particularly important in light of the counterintuitive observation that noncoronary sinus CRT-D systems had a higher risk for dislodgement when compared with coronary sinus systems. It may be that additional manipulation of the device system increased the risk of other leads to dislodge, rather than concluding that the noncoronary sinus lead was more unstable. Lastly, no data were collected on other factors such as implant techniques, patient's body habitus, procedural times, and post-operative management (i.e., arm sling use, limitations in arm movement).
Conclusions
Acute lead dislodgement was the most common adverse event reported. Physician training was important in determining its outcome, and our findings call into question the ability of alternative training pathways in achieving a comparable degree of expertise as compared with more formalized methods. Heightened awareness for other adverse events should be made in the presence of acute dislodgements given that 10.9% of cases were also associated with another type of complication, including in-hospital death.
1. : "Complications of pacemakers and defibrillators in the elderly". Am J Geriatr Cardiol 2006; 15: 102.
2. : "Patient, procedural and hardware factors associated with pacemaker lead failures in pediatrics and congenital heart disease". Heart Rhythm 2004; 1: 150.
3. : "The additional hospital costs generated in the management of complications of pacemaker and defibrillator implantations". J Thorac Cardiovasc Surg 1996; 111: 742.
4. : "Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction". N Engl J Med 2002; 346: 877.
5. : "Cardiac-resynchronization therapy for the prevention of heart-failure events". N Engl J Med 2009; 361: 1329.
6. : "Increased incidence of subacute lead perforation noted with one implantable cardioverter-defibrillator". Heart Rhythm 2007; 4: 439.
7. : "Rates and severity of perforation from implantable cardioverter-defibrillator leads: a 4-year study". J Interv Card Electrophysiol 2009; 24: 47.
8. : "Safety of transvenous cardiac resynchronization system implantation in patients with chronic heart failure". J Am Coll Cardiol 2005; 46: 2348.
9. : "Review of the ICD registry's third year, expansion to include lead data and pediatric ICD procedures, and role for measuring performance". Heart Rhythm 2009; 6: 1397.
10. : "The relation between patients' outcomes and the volume of cardioverter-defibrillator implantation procedures performed by physicians treating Medicare beneficiaries". J Am Coll Cardiol 2005; 46: 1536.
11. : "Clinical competency statement: training pathways for implantation of cardioverter defibrillators and cardiac resynchronization devices". Heart Rhythm 2004; 1: 371.
12. : "Early LV lead dislodgement related to hyperpnea respiration". PACE 2006; 29: 425.
13. : "Evaluation of early complications related to de novo cardioverter defibrillator implantation". J Am Coll Cardiol 2010; 55: 774.
Abbreviations and Acronyms
| CRT-D | cardiac resynchronization therapy-defibrillator |
| EP | electrophysiology |
| ICD | implantable cardioverter-defibrillator |
| LV | left ventricular |
| NCDR | National Cardiovascular Data Registry |
| NYHA | New York Heart Association |
Footnotes
This work was supported by the
{kind=link}