Influence of Microvascular Disease on Cardiovascular Events in Type 2 Diabetes
Letters
Introduction
In people with type 2 diabetes (T2D), the presence of microvascular disease is associated with increased risk for macrovascular events (1). Of particular interest is whether microvascular disease is a risk factor for heart failure (HF) or has a role in its pathophysiology (2). The relationship of microvascular disease to HF and other cardiovascular outcomes has not been studied in the context of contemporary cardiovascular outcomes trials (CVOTs). In the EMPA-REG OUTCOME CVOT (BI 10773 [Empagliflozin] Cardiovascular Outcome Event Trial in Type 2 Diabetes Mellitus Patients), empagliflozin reduced the risk of 3-point major adverse cardiovascular events (MACE)—cardiovascular death, nonfatal myocardial infarction, or nonfatal stroke—by 14% compared with placebo (hazard ratio [HR]: 0.86; 95% confidence interval [CI]: 0.74 to 0.99), hospitalization for heart failure (HHF) by 35% (HR: 0.65; 95% CI: 0.50 to 0.85), and the composite of cardiovascular death or HHF by 34% (HR: 0.66; 95% CI: 0.55 to 0.79) (3). In the present analysis, we examined the risk of microvascular disease on cardiovascular outcomes, including HHF, in EMPA-REG OUTCOME, and compared the effect of empagliflozin in individuals with/without microvascular disease.
The design of EMPA-REG OUTCOME ( NCT01131676) has been described previously (3). Briefly, adults with T2D, glycated hemoglobin 7% to 10%, and established cardiovascular disease were randomized 1:1:1 to empagliflozin, 10 or 25 mg, or placebo added to standard of care, and were treated until ≥691 participants had experienced an adjudicated primary outcome event (3-point MACE). In subgroups categorized by investigator-reported history of microvascular disease at baseline (≥1 of retinopathy, neuropathy, or nephropathy), we assessed post hoc the risk of 3-point MACE, HHF, and cardiovascular death or HHF in those who received ≥1 dose of study drug, using Cox proportional hazards models. The model for the placebo group included terms for age, sex, baseline body mass index, baseline glycated hemoglobin, baseline estimated glomerular filtration rate, region, and baseline microvascular conditions, and the model comparing empagliflozin and placebo contained additional terms for treatment and treatment-by-microvascular-disease-at-baseline interaction.
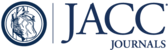
Of the 7,020 EMPA-REG OUTCOME participants, 3,420 (48.7%) had pre-existing microvascular disease (Figure 1A). These individuals, compared with those without microvascular disease, had longer T2D duration (>10 years in 69.4% vs. 45.5%), lower estimated glomerular filtration rate (mean 70.76 ml/min/1.73 m2 vs. 77.17 ml/min/1.73 m2, and more prevalent insulin use (63.0% vs. 34.3%) and HF (12.5% vs. 7.8%), but otherwise generally similar baseline characteristics.

Prevalence of Microvascular Disease at Baseline in EMPA-REG OUTCOME, and its Influence on Cardiovascular Effects of Empagliflozin
(A) EMPA-REG OUTCOME participants with baseline microvascular disease. (B) Influence of microvascular disease on cardiovascular effects of empagliflozin. ∗Participants with ≥2 microvascular diseases at baseline. †p values for treatment-by-subgroup interaction were obtained from tests of homogeneity of treatment-group differences among subgroups without adjustment for multiple testing. ‡Excluding fatal stroke. CI = confidence interval; CV = cardiovascular; HHF = hospitalization for heart failure; HR = hazard ratio; MACE = major adverse cardiovascular events (cardiovascular death, nonfatal myocardial infarction, nonfatal stroke).
In the placebo group, the presence of any microvascular disease at baseline was associated with higher risk for subsequent HHF (HR: 1.63; 95% CI: 1.06 to 2.49; p = 0.0245) and cardiovascular death or HHF (HR: 1.30; 95% CI: 0.97 to 1.73; p = 0.0751), but not 3-point MACE (HR: 1.16; 95% CI: 0.92 to 1.48; p = 0.2144). Furthermore, with increasing numbers of microvascular diseases, there was a trend toward worsening HF outcomes: for participants with 1, 2, or 3 microvascular diseases, the HRs for HHF were 1.34, 1.46, and 3.88, respectively (p for trend = 0.0003), compared with those without microvascular disease, while the respective HRs for cardiovascular death or HHF were 1.13, 1.08, and 2.91 (p for trend = 0.0007). For 3-point MACE, the HRs showed the same directionality (1.09, 1.15, 1.65; p for trend = 0.0552), indicating additional risk of cardiovascular events in this high-risk population with increasing numbers of microvascular diseases. Risk reductions with empagliflozin compared with placebo for these outcomes were consistent between patients with or without microvascular disease (Figure 1B).
One limitation of our analyses is that participants with microvascular abnormalities without clinical manifestations may not have been classified as having microvascular disease.
In conclusion, in people with T2D, the coexistence of microvascular disease in the setting of established macrovascular disease is associated with increased cardiovascular risk, including—notably—HHF, which has hitherto been underappreciated. The cardiovascular benefit of empagliflozin in this population was consistent with its effects in people without microvascular disease. These findings from a large modern CVOT add to the limited prospective data on the effect of microvascular disease on cardiovascular and HF outcomes in people with T2D.
1. : "Microvascular disease and risk of cardiovascular events among individuals with type 2 diabetes: a population-level cohort study". Lancet Diabetes Endocrinol 2016; 4: 588.
2. : "Diabetic retinopathy and risk of heart failure". J Am Coll Cardiol 2008; 51: 1573.
3. : "Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes". N Engl J Med 2015; 373: 2117.
Footnotes
Please note: The EMPA-REG OUTCOME trial was funded by the Boehringer Ingelheim and Eli Lilly and Company Diabetes Alliance. Employees of the funder who are authors of this paper were involved in the design and conduct of the study; in the collection, analysis, and interpretation of the data; and in the preparation, review, and approval of the manuscript. Dr. Verma is the President of the Canadian Medical and Surgical Knowledge Translation Research Group, a federally incorporated not-for-profit physician organization; holds a Tier 1 Canada Research Chair in Cardiovascular Surgery; and has received research grants and/or speaking honoraria from Boehringer Ingelheim/Lilly, AstraZeneca, Janssen, Merck, Novartis, Novo Nordisk, Amgen, Sanofi, Servier, Valeant, Bayer, and Pfizer. Dr. Wanner has received honoraria from AstraZeneca, Boehringer Ingelheim, Eli Lilly, Merck Sharp & Dohme, Mitsubishi, and Sanofi; and has served as a lecturer and on Steering Committees for Boehringer Ingelheim. Drs. Zwiener, Ofstad, and George are employees of Boehringer Ingelheim. Dr. Fitchett has received honoraria from Sanofi, Merck & Co., Amgen, AstraZeneca, Eli Lilly and Company, and Boehringer Ingelheim. Dr. Zinman has received research grants awarded to his institution from Boehringer Ingelheim, AstraZeneca, and Novo Nordisk; and has received honoraria from Janssen, Sanofi, Eli Lilly and Company, Boehringer Ingelheim, Novo Nordisk, and Merck. Medical writing assistance, supported financially by Boehringer Ingelheim, was provided by Giles Brooke, PhD, CMPP, of Elevate Scientific Solutions during the preparation of this manuscript. (BI 10773 [Empagliflozin] Cardiovascular Outcome Event Trial in Type 2 Diabetes Mellitus Patients [EMPA-REG OUTCOME]; NCT01131676)
{kind=link}