Atrial fibrillation and atrial vulnerability in patients with Brugada syndrome
Clinical study: cardiac arrhythmias
Abstract
Objectives:
We sought to study atrial vulnerability in patients with Brugada syndrome.
Background:
Atrial fibrillation (AF) often occurs in patients with Brugada syndrome, but atrial vulnerability in Brugada syndrome has not been evaluated.
Methods:
The patient group consisted of 18 patients with Brugada syndrome. The control group consisted of 12 age- and gender-matched subjects who had neither organic heart disease nor AF episodes. The incidence and clinical characteristics of AF were evaluated in all 18 patients with Brugada syndrome, and an electrophysiologic study was performed in all 12 control subjects and in 14 of the 18 patients with Brugada syndrome. The atrial effective refractory period of the right atrium (RA-ERP), intra-atrial conduction time (conduction time from the stimulus at the right atrium to atrial deflection at the distal portion of the coronary sinus), duration of local atrial potential, and repetitive atrial firing (occurrence of two or more premature atrial complexes after atrial stimulation) were studied.
Results:
Spontaneous AF occurred in 7 of the 18 patients with Brugada syndrome but in none of the control subjects. The RA-ERP was not different between the two groups. The intra-atrial conduction time was increased in the Brugada syndrome group versus the control group (168.4 ± 17.5 vs. 131.8 ± 13.0 ms, p < 0.001). The duration of atrial potential at the RA-ERP was prolonged in the Brugada syndrome group versus the control group (80.3 ± 18.0 vs. 59.3 ± 9.2 ms, p < 0.001). Repetitive atrial firing was induced in nine patients with Brugada syndrome and in six control subjects. Atrial fibrillation was induced in eight patients with Brugada syndrome but in none of the control subjects. In patients with Brugada syndrome without spontaneous AF, the intra-atrial conduction time and duration of atrial potential were also increased.
Conclusions:
Atrial vulnerability is increased in patients with Brugada syndrome. Abnormal atrial conduction may be an electrophysiologic basis for induction of AF in patients with Brugada syndrome.
Introduction
The Brugada syndrome is characterized by ST-segment elevation in leads V1 to V3 with a right bundle branch block pattern and nocturnal sudden cardiac death due to ventricular fibrillation (1–5).
Arrhythmias such as premature ventricular contraction, monomorphic ventricular tachycardia, polymorphic ventricular tachycardia (6–8), and ventricular fibrillation have been reported. In addition, atrial arrhythmia has also been reported in patients with Brugada syndrome (2,9–13). Recently, it has been reported that mutations of the sodium channel gene cause Brugada syndrome (4–19). If Brugada syndrome is a sodium channel disease, it is possible that an electrical abnormality of the myocardium might exist not only in the ventricular myocardium (5,20) but also in the atrial myocardium. Thus, in this study, we evaluated atrial vulnerability in patients with Brugada syndrome.
Methods
Patients
Patients
The patient group consisted of 18 patients with Brugada syndrome (Table 1). The patients were all men, ranging in age from 33 to 71 years (mean 49 ± 11). All of the patients with Brugada syndrome showed the typical electrocardiographic (ECG) “Brugada sign,” which was defined previously (4). Ten patients with Brugada syndrome had experienced syncopal episodes or had a family history of sudden cardiac death. The other eight patients were asymptomatic and had no family history of sudden cardiac death. The control group consisted of 12 age- and gender-matched subjects (mean age 48 ± 10 years [range 35 to 60]) who had no sign of the Brugada-type ECG change and no episodes of atrial fibrillation (AF), nor could AF be induced by programmed electrical stimulation. The 12 subjects in the control group included 9 patients with paroxysmal supraventricular tachycardia without manifest Wolf-Parkinson-White syndrome and 3 patients with idiopathic ventricular tachycardia.
| Pt. No. | Age | Gender | EPS | VF/Syncope* | Family History† | VA Induction‡ | AF (Spont.)§ | AF (EPS)∥ | Therapy | Follow-Up(month) | AFFrequency |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 33 | M | + | + | + | + | − | − | ICD | 18 | 0 |
| 2 | 36 | M | + | − | − | + | − | − | None | 18 | 0 |
| 3 | 39 | M | + | − | − | + | − | − | ICD | 16 | 0 |
| 4 | 40 | M | + | − | − | + | − | + | None | 60 | 0 |
| 5 | 41 | M | + | + | + | + | − | − | ICD | 63 | 0 |
| 6 | 41 | M | + | − | − | + | − | + | ICD | 27 | 0 |
| 7 | 45 | M | + | + | + | + | − | + | ICD | 12 | 0 |
| 8 | 51 | M | + | − | − | − | − | + | None | 72 | 0 |
| 9 | 52 | M | + | − | − | − | − | − | None | 48 | 0 |
| 10 | 55 | M | + | + | + | + | − | + | ICD + Disopyramide | 38 | 0 |
| 11 | 45 | M | + | + | − | + | − | + | ICD | 130 | 0 |
| 12 | 42 | M | + | − | − | + | + | + | None | 23 | 1 |
| 13 | 55 | M | + | + | − | + | + | + | ICD + Disopyramide | 22 | 1 |
| 14 | 55 | M | − | − | + | NA | + | NA | None | 53 | 1/M |
| 15 | 56 | M | − | + | + | NA | + | NA | None | 36 | 2 |
| 16 | 58 | M | + | + | + | + | + | − | ICD | 17 | 3 |
| 17 | 70 | M | − | − | − | NA | + | NA | None | 12 | 4 |
| 18 | 71 | M | − | + | − | NA | + | NA | ICD | 40 | 8 |
Study protocol
Evaluation of incidence of AF
Evaluation of incidence of AF
The occurrence of AF was evaluated by clinical follow-up (every month), observing the patient’s symptoms, and 24-h Holter ambulatory ECG recording. Continuous ECG monitoring was performed from two to three weeks during administration.
Electrophysiologic study
After obtaining the patients’ written, informed consent, an electrophysiologic study was performed in all 12 control subjects and in 14 of 18 patients with Brugada syndrome. After right femoral and right carotid venous access was obtained, three quadripolar electrode catheters (6F) with an interelectrode distance of 5 mm (EP Technologies, Boston Scientific, Inc., Sunnyvale, California) were positioned in the right atrial appendage (RAA), His bundle region, and right ventricle, and an octopolar catheter (6F) with an interelectrode distance of 2.5 mm (EP Technologies, Boston Scientific, Inc.) was positioned into the coronary sinus (CS). Endocardial po-tentials were recorded by bipolar and filtered to record frequencies of 30 to 400 Hz. Programmed electrical stimulation was performed at an intensity of twice the threshold and for 2 ms in duration through the distal electrodes in the RAA, using the SEC3105 Nihon-Koden pulse generator. A premature stimulus (S2) was delivered after eight beats of drive pacing (S1) at a basic cycle length of 600 ms. The S1–S2 interval was decreased in 10-ms steps until the effective refractory period (ERP) of the RAA was reached. The first deflection in amplified recordings of the atrial electrograms was taken as the onset of atrial depolarization.
Atrial vulnerability was evaluated by the ERP of the RAA, intra-atrial conduction time (CT) and conduction delay (CD) during the basic cycle length of S1 and extrastimulus of S2, duration of the local right atrial potential during the basal cycle length of S1 and extrastimulus of S2, and repetitive atrial firing (RAF) and induced AF in response to S2.
The occurrence of premature atrial contraction (PAC) and AF was evaluated at baseline and after infusion of 2 μg isoproterenol in all control subjects and patients with Brugada syndrome in whom an electrophysiologic study had been performed.
Definitions
The ERP was defined as the longest coupling interval (S1–S2) at which the stimulus failed to propagate a response. The intra-atrial CT was defined as the interval from the stimulus to the atrial deflection at the distal portion of the CS. The CD was defined as the difference between the CT at S2 and that at S1, and a positive CD was defined as an increase of ≥20 ms in CT at S2 compared with that at S1. The CD zone was defined as the range of the coupling interval that shows a positive CD (21–23).
The presence of fragmented atrial activity (FAA) was defined as the duration of A2 at the ERP of RAA/duration of A1 ≥150%. The FAA zone was defined as the range of the coupling interval that resulted in FAA (24–26). Repetitive atrial firing was defined as the occurrence of two or more premature atrial complexes (21,22).
Induced AF was defined as AF that was induced by programmed electrical stimulation and persisted for >30 s. Spontaneous AF was defined as AF detected by 12-lead electrocardiography or ambulatory ECG monitoring without any maneuvers, including programmed electrical stimulation and drug stress tests.
Statistical analysis
Quantitative data are expressed as the mean value ± SD. The statistical significance of the differences was analyzed by using the Student t test for unpaired values. A value of p < 0.05 was considered as statistically significant.
Results
Clinical characteristics and incidence and frequency of AF in patients with Brugada syndrome
Clinical characteristics and incidence and frequency of AF in patients with Brugada syndrome
Spontaneous paroxysmal AF was detected in 7 (39%) of 18 patients with Brugada syndrome: 5 with ventricular fibrillation or a positive family history of sudden death and 2 asymptomatic patients with Brugada syndrome and no family history of sudden death. All patients had a paroxysmal attack of AF, and none of the patients showed persistent or chronic AF. The frequency of AF attack was low in the majority of patients with Brugada syndrome (Table 1). The patients’ mean age of AF onset was 56 ± 11 years.
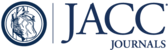
The Holter ambulatory ECG showed that PAC rarely occurred in patients with Brugada syndrome; mean, median, and range of PACs were 5 ± 6, 12, and 0 to 23/day, respectively. Initiation of AF was detected in Patient 18 only; AF was followed by rapid firing of PAC, but no PACs were observed before the occurrence of AF (Fig. 1).

Initiation of spontaneous atrial fibrillation (AF) on the Holter ambulatory electrocardiogram. (a) Spontaneous AF occurred at midnight. Premature atrial contraction was not observed before the occurrence of AF. (b) Initiation of paroxysmal AF. Paroxysmal atrial contraction occurred on the T-wave at the initiation of AF. Coarse fibrillatory waves succeeded and degenerated into fine and irregular f waves.
Isoproterenol infusion
Isoproterenol infusion did not induce any PACs or AF in the control subjects. Isoproterenol infusion induced PAC and AF in only one patient with Brugada syndrome (Patient 18), but neither PAC nor AF occurred in any of the other patients.
Atrioventricular conduction
The ventricular response during spontaneous AF in patients with Brugada syndrome was relatively slow (Fig. 2); the mean heart rate during AF was 63 ± 10 beats/min.

Spontaneous atrial fibrillation (AF) in patients with Brugada syndrome. Note the slower ventricular response during AF. Lead V2 is shown.
The AH interval was significantly prolonged (p < 0.001) in the Brugada syndrome group (96.9 ± 10.6 ms), as compared with that in the control group (73.8 ± 15.3 ms). The HV interval was prolonged in the Brugada syndrome group, but not significantly so (41.3 ± 6.7 vs. 36.2 ± 6.5 ms in control group, p = 0.057). The ERP of atrioventricular node was prolonged in patients with Brugada syndrome (350.7 ± 69.9 vs. 271.8 ± 42.0 ms in control group, p < 0.001) (Fig. 2). The one-to-one conduction of the atrioventricular node was slower in the Brugada syndrome group (133 ± 17 beats/min) than in the control group (173 ± 31 beats/min, p < 0.01).
Induction of RAF and AF
Repetitive atrial firing was induced in nine patients with Brugada syndrome (64.3%) and in six control subjects (50%), and there was no significant difference between the two groups. However, AF was induced in 8 (57.1%) of 14 patients with Brugada syndrome and in none of the control subjects.
Atrial vulnerability
There was no significant difference between the ERP of the RA in the Brugada syndrome group and that in the control group (247.1 ± 27.0 vs. 243.3 ± 20.6 ms) (Fig. 3).

Effective refractory period of the atrioventricular node (a) and right atrium (RA) (b). (a) The effective refractory period (ERP) of atrioventricular node was prolonged in the Brugada syndrome patients with and without atrial fibrillation (AF). (b) There was no significant difference between the ERP of the RA in the Brugada syndrome group and that in the control group. There was also no significant difference between the ERP of the RA in the Brugada syndrome patients without AF and that in the control group. Open circles show the Brugada syndrome group with spontaneous AF. Solid circles show the Brugada syndrome patients without spontaneous AF. The error bars represent the 95% confidence interval. NS = not significant.
There was no significant difference between the CT at S1 (CT1) in patients with Brugada syndrome and that in the control group (119.4 ± 15.7 vs. 110.1 ± 19.1 ms), but the CT at S2 (CT2) in the Brugada syndrome group was markedly delayed (168.4 ± 17.5 vs. 131.8 ± 13.0 ms in control group, p < 0.001) (Fig. 4).

(a) Conduction time (CT) at S1 and (b) CT at S2. There was no difference between the CT at S1 in patients with Brugada syndrome and that in the control group, but the CT at S2 in the Brugada syndrome group was markedly delayed at the right atrium-effective refractory period. The CT1 in the Brugada syndrome patients without atrial fibrillation (AF) was not different from that in the control group, but the CT2 in these Brugada syndrome patients was prolonged. (c) Inter-atrial conduction delay. The conduction delay (CD) was markedly prolonged in the Brugada syndrome group, and all patients with Brugada syndrome showed a positive CD. The CD was also prolonged in the Brugada syndrome patients without AF. Open circles show the Brugada syndrome patients with spontaneous AF. Solid circles show the Brugada syndrome patients without spontaneous AF. The error bars represent the 95% confidence interval.
All of the patients with Brugada syndrome had a positive CD (49.0 ± 13.7 vs. 21.8 ± 12.2 ms in control group, p < 0.001) (Fig. 3). The CD zone was markedly wider in the Brugada syndrome group than in the control group (37.1 ± 14.4 vs. 20.0 ± 11.0 ms, p < 0.05).
There was no significant difference between the duration of A1 in patients with Brugada syndrome and that in the control group (51.3 ± 6.0 vs. 49.9 ± 5.3 ms in control group), but the A2 in the Brugada syndrome group was markedly prolonged compared with that in control group (80.3 ± 18.0 vs. 59.3 ± 9.2 ms, p < 0.01) (Fig. 5). The prolongation of A2 compared with A1 was more prominent in the Brugada syndrome group than in the control group (156.5 ± 27.8% vs. 118.8 ± 12.5%, p < 0.001) (Fig. 4). Half of the patients with Brugada syndrome showed positive FAA, but only one patient in the control group showed positive FAA. The FAA zone was wider in Brugada syndrome (43.0 ± 25.8 ms).

Duration of atrial potential and fragmented atrial activity (FAA). (a) Duration of A1. There was no difference between the duration of A1 in patients with Brugada syndrome and that in the control group. (b) Duration of A2. The duration of A2 in Brugada syndrome was markedly prolonged compared with that in the control group. The duration of A2 was also markedly prolonged in Brugada syndrome patients without atrial fibrillation (AF). (c) FAA. The ratio of the duration of A2 to A1 in the Brugada syndrome group was prolonged compared with that in the control group, and half of the patients with Brugada syndrome showed positive FAA, whereas only one patient in the control group showed positive FAA. The A2/A1 ratio was also prolonged in Brugada syndrome patients without AF. Open circles show Brugada syndrome patients with spontaneous AF. Solid circles show Brugada syndrome patients without spontaneous AF. The error bars represent the 95% confidence interval.
Brugada syndrome patients without a spontaneous AF attack
Atrial vulnerability in the 11 Brugada syndrome patients who had no spontaneous AF attack was evaluated. There was no difference between the ERP of RA in the Brugada syndrome group without AF and that in the control group (243.6 ± 28.7 vs. 243.3 ± 20.6 ms). The indexes of atrial conduction (CT2, CD, and CD zone) were prolonged in the Brugada syndrome group without AF (CT2: 164.5 ± 17.8 ms; CD: 47.3 ± 14.1 ms; CD zone: 37.3 ± 16.2 ms; p < 0.05) compared with the control group. The indexes of local atrial potential were also prolonged in the Brugada syndrome group without AF (A2: 82.5 ± 19.3 ms; A2/A1: 159.3 ± 30.8%; FAA zone: 48.8 ± 25.9 ms; p < 0.0001). In the Brugada syndrome group without AF, RAF was induced in seven patients (63.6%), and AF was induced in six patients (54.5%). In all figures, the data of the Brugada syndrome patients without spontaneous AF are represented by solid circles.
Discussion
Polymorphic ventricular tachycardia and ventricular fibrillation in patients with Brugada syndrome may be lethal, and the implantable cardioverter-defibrillator is necessary for the treatment of Brugada syndrome (1,2). Recently, it has been shown that mutations in the cardiac sodium channel gene, which result in slow recovery from inactive states of the sodium channel or sodium channel dysfunction, cause Brugada syndrome (14–18). This functional change in the mutational sodium channel will explain the conduction abnormality of the ventricle and the easy inducibility of ventricular fibrillation (19), the late activation in the right ventricular outflow tract, and the abnormal late potential (20). If a mutation in the cardiac sodium channel does in fact cause Brugada syndrome (14–16,19), a myocardial electrical abnormality might exist not only in the ventricular myocyte but also in the atrial myocyte. We therefore evaluated the incidence of AF and electrical abnormality in the atrium in Brugada syndrome. In this study, we found that atrial vulnerability was enhanced, and the incidence of AF was increased in patients with Brugada syndrome.
Incidence of AF in Brugada syndrome
Some reports demonstrated the ECGs of AF in patients with Brugada syndrome (1–4,10–13), but the exact incidence of AF in patients with Brugada syndrome is not known. Anzelevitch et al. (2) reported that only 10% of patients with Brugada syndrome exhibit paroxysmal AF. In the present study, the incidence of spontaneous AF in patients with Brugada syndrome was high (39%), and the incidence of AF induced by electrical stimulation was also high. These results show that AF is not rare in patients with Brugada syndrome.
Spontaneous PACs on the Holter ambulatory ECG recording were rare in our Brugada syndrome group. Isoproterenol infusion induced AF in only one patient, but PAC and AF were not induced by isoproterenol infusion in the other patients. Therefore, we were not able to evaluate the trigger of AF and its foci (28,29). Our study indicates that the incidence of AF in patients with Brugada syndrome was high, but the frequency of AF attack in each patient was low. This suggests that the substrate of AF (that is, abnormal atrial vulnerability) exists and results in random reentry in the atrium, but the trigger of AF (i.e., PAC) is rare in patients with Brugada syndrome.
Characteristics of AF and atrioventricular conduction in Brugada syndrome
Because the ventricular response during paroxysmal AF was not rapid in patients with Brugada syndrome, it was thought that the atrioventricular conduction was decreased. Furthermore, ECG recordings of AF in some reports have shown a slow ventricular response during AF, and the HV interval was also prolonged in patients with Brugada syndrome (1,3,11,12). In the present study, the patients with Brugada syndrome showed slower one-to-one atrioventricular conduction, as measured by atrial pacing, as compared with the control group, and the AH and HV intervals and ERP of the atrioventricular node were prolonged in patients with Brugada syndrome. Slow atrioventricular conduction results in a slow ventricular response during AF. Because it is believed that vagal activity plays an important role in ST-segment elevation and the occurrence of ventricular fibrillation in patients with Brugada syndrome (5), the vagal activity might be related to the initiation of paroxysmal AF and slower atrioventricular conduction in patients with Brugada syndrome. It has been reported that cardiac sodium channel mutations caused the long QT syndrome, Brugada syndrome, and cardiac conduction disease. Because the sodium channel mutation reported in Brugada syndrome showed sodium channel dysfunction, such an abnormal sodium channel would cause an atrioventricular conduction disturbance (27).
Atrial vulnerability in Brugada syndrome
Atrial vulnerability indicates injured atrial myocardial electrical function that would cause a reentrant circuit. Abnormal atrial vulnerability has been found in patients with atrial arrhythmia associated with sick sinus syndrome (21,24,25) and Wolf-Parkinson-White syndrome (22). The index of atrial vulnerability (21–26,30) includes intra-atrial CD, FAA, RAF, and atrial refractoriness. The intra-atrial CD indicates global conduction of the atrial myocardium—that is, a change in the CT during a stimulus of a constant drive train and extrastimulus from the right atrium to the left lateral atrium through the inter-atrial septum. The FAA indicates local atrial CD—that is, discontinuous propagation and slowed conduction in a local atrial site. For induction and persistence of AF, the tissue wavelength determines the minimal size of a reentrant wavelet, and the persistence of AF depends on the average total number of wavelets the tissue can support; intra-atrial and local atrial CD and atrial refractoriness were also important.
The present study demonstrated that atrial vulnerability, especially the index of intra-atrial and local atrial conduction abnormality, was enhanced in patients with Brugada syndrome. Atrial vulnerability was enhanced not only in Brugada syndrome patients with AF, but also in Brugada syndrome patients without AF. Thus, an electrical abnormality of the atrium existed in patients with Brugada syndrome who did not experience an attack of AF. Thus, atrial electrical abnormality existed in Brugada syndrome patients without AF. The atrial ERPs were not different in patients with Brugada syndrome. These results show that a conduction abnormality is important for the occurrence of AF in patients with Brugada syndrome. The occurrence of RAF in patients with Brugada syndrome indicates that the atrial conduction abnormality easily induces the reentrant circuit. Clinically, patients with Brugada syndrome showed easy inducibility of ventricular fibrillation by programmed electrical stimulation and a conduction abnormality within the ventricle. It is possible that similar genetic defects alter atrial and ventricular electrophysiology in these patients with Brugada syndrome.
Clinical implications
This study showed that atrial vulnerability was enhanced and that the occurrence of paroxysmal AF was frequent in patients with Brugada syndrome. The implantable cardioverter-defibrillator could detect AF on the electrogram as ventricular fibrillation and would start cardioversion. The fifth-generation implantable cardioverter-defibrillator is preferred for patients with Brugada syndrome, even those who have not experienced an attack of AF, because atrial vulnerability is common and AF could occur during the follow-up period.
Conclusions
This study showed that: 1) the incidences of spontaneous and induced AF in patients with Brugada syndrome were high; 2) atrial vulnerability was increased in patients with Brugada syndrome; and 3) atrial vulnerability was also increased in the Brugada syndrome patients without spontaneous AF. Abnormal atrial conduction may play an important role in the induction of AF in patients with Brugada syndrome.
1. : "Right bundle branch block, persistent ST segment elevation and sudden cardiac death: a distinct clinical and electrocardiographic syndrome". J Am Coll Cardiol 1992; 20: 1391.
2. Anzelevitch C, Brugada P, Brugada J, et al. The Brugada syndrome. In: Camm AJ, editor. Clinical Approaches to Tachyarrhythmias. Armonk, NY: Futura, 1999
3. : "Early repolarization syndrome: clinical characteristics and possible cellular and ionic mechanism". J Electrocardiol 2000; 33: 299.
4. : "Relatively benign clinical course in asymptomatic patients with Brugada-type electrocardiogram without family history of sudden death". J Cardiovasc Electrophysiol 2001; 12: 2.
5. : "The idiopathic ventricular fibrillation induced with vagal activity in patients without obvious heart disease". Circulation 1997; 95: 2277.
6. : "Sustained monomorphic ventricular tachycardia in a patient with Brugada syndrome". Jpn Circ J 1996; 60: 364.
7. : "Incomplete bundle branch block and ST-segment elevation: syndrome associated with sustained monomorphic ventricular tachycardia in patients with apparently normal heart". Clin Cardiol 1997; 20: 407.
8. : "Brugada syndrome: a case report of monomorphic ventricular tachycardia". Pacing Clin Electrophysiol 2001; 24: 112.
9. : "Brugada syndrome and supraventricular tachyarrhythmias: a novel association?". J Cardiovasc Electrophysiol 2001; 12: 680.
10. : "Prevention of ventricular fibrillation by pacing in a man with Brugada syndrome". J Cardiovasc Electrophysiol 2000; 11: 935.
11. : "ST segment elevation in the right precordial leads induced with class Ic antiarrhythmic drugs: insight into the mechanism of Brugada syndrome". J Cardiovasc Electrophysiol 1999; 10: 214.
12. : "Dynamic changes of 12-lead electrocardiograms in a patient with Brugada syndrome". J Cardiovasc Electrophysiol 1998; 9: 508.
13. : "Safety and efficacy of oral flecainide acetate in patients with cardiac arrhythmias". Jpn Heart J 1997; 38: 379.
14. : "Genetic basis and molecular mechanisms for idiopathic ventricular fibrillation". Nature 1998; 392: 293.
15. : "Human SCN5A gene mutations alter cardiac sodium channel kinetics and are associated with the Brugada syndrome". Cardiovasc Res 1999; 44: 507.
16. : "Sodium “channelopathies” and sudden death: must you be so sensitive?". Circ Res 1999; 85: 872.
17. : "Cardiac sodium channel and inherited arrhythmia syndromes". Cardiovasc Res 2001; 49: 257.
18. : "Electrical heterogeneity, cardiac arrhythmias and the sodium channel". Circ Res 2000; 87: 964.
19. : "Ventricular tachycardia or conduction disease: what is the mechanism of death associated with SCN5A?". J Cardiovasc Electrophysiol 2001; 12: 637.
20. : "Assessment of noninvasive markers in identifying patients at risk in the Brugada syndrome: insight into risk stratification". J Am Coll Cardiol 2001; 37: 1628.
21. : "Intra-atrial conduction delay and fragmented atrial activity in patients with paroxysmal atrial fibrillation". Jpn Cic J 1989; 53: 1023.
22. : "Electrophysiologic characteristics of human atrial muscle in paroxysmal atrial fibrillation". Am Heart J 1996; 131: 778.
23. : "Identification of the substrate of atrial vulnerability in patients with idiopathic atrial fibrillation". Circulation 2000; 101: 995.
24. : "Relation between the widening of the fragmented atrial activity zone and atrial fibrillation". Am J Cardiol 1983; 53: 1219.
25. : "The effects of cycle length on the fragmented atrial activity zone in patients with sick sinus syndrome". J Electrocardiol 1987; 20: 364.
26. : "Prolonged fractionation of paced right atrial electrograms in patients with atrial flutter and fibrillation". J Am Coll Cardiol 2001; 37: 1651.
27. : "Clinical, genetic, and biophysical characterization of SCN5A mutations associated with atrioventricular conduction block". Circulation 2002; 105: 341.
28. : "Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins". N Engl J Med 1998; 339: 659.
29. : "Initiation of atrial fibrillation by ectopic beats originating from the pulmonary veins: electrophysiological characteristics, pharmacological responses, and effects of radiofrequency ablation". Circulation 1999; 100: 1879.
30. : "Electrophysiological properties of human atrium in atrial fibrillation". Cardiovasc Res 2002; 54: 302.
Abbreviations
| AF | atrial fibrillation |
| CD | conduction delay |
| CS | coronary sinus |
| CT | conduction time |
| ERP | effective refractory period |
| FAA | fragmented atrial activity |
| PAC | premature atrial contraction |
| RA | right atrium/atrial |
| RAA | right atrial appendage |
| RAF | repetitive atrial firing |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}