Hemodynamic and Cardiac Effects of the Selective T-Type and L-Type Calcium Channel Blocking Agent Mibefradil in Patients With Varying Degrees of Left Ventricular Systolic Dysfunction1
Abstract
Objectives. This study sought to assess the hemodynamic and cardiac effects of two dose levels of mibefradil in patients with varying degrees of ischemic left ventricular dysfunction.
Background. Mibefradil is a new, selective T-type and L-type calcium channel blocking agent. Because L-type channel blockade may depress myocardial performance, an invasive hemodynamic study was performed to assess the safety of this agent.
Methods. We performed an open label study, examining the effects of two intravenous doses of mibefradil, selected to produce plasma levels comparable to those measured after oral administration of 50 mg (dose 1: 400 ng/ml) or 100 mg (dose 2: 800 ng/ml) of the drug. Variables studied included the indexes of left ventricular function and neurohormone levels. Patients were stratified according to ejection fraction (EF) (≥40%, n = 26; <40%, n = 24) and the presence (n = 15) or absence (n = 35) of heart failure.
Results. In patients with preserved systolic function, dose 1 had no clinically significant hemodynamic effects, but dose 2 decreased mean aortic pressure and systemic vascular resistance (−8.5 mm Hg, −12%, both p < 0.01) and also reduced end-systolic stress and volume, thus improving EF (52% to 58%, p < 0.01). Heart rate tended to decrease. In patients with depressed EF, heart rate decreased significantly with both doses. The effects of dose 1 mimicked those observed after dose 2 in patients with preserved EF. Dose 2 (plasma levels 1,052 ± 284 ng/ml) still decreased left ventricular systolic wall stress and improved EF (24.0% to 28.5%, p < 0.05) but also significantly depressed the maximal first derivative of left ventricular pressure. Examination of individual pressure-volume loops in two patients with heart failure showed a clear rightward shift of the loop despite a decrease in systolic pressure, suggesting negative inotropy. Neurohormone levels were unchanged at both dose levels and in all subgroups.
Conclusions. Intravenous mibefradil was well tolerated and produced an overall favorable cardiovascular response. However, high plasma concentrations might produce myocardial depression in patients with heart failure, and caution should be exerted in this setting.
Introduction
It is widely recognized that several formulations of calcium channel blocking agents are of no benefit and may even be harmful in acute coronary syndromes [1, 2]and in congestive heart failure [3, 4]. Controversy also exists regarding the long-term use of these agents in chronic stable angina or hypertension [5–7]. Before any conclusions are drawn as to the safety and effectiveness of calcium channel blockers, it is important to realize that the term “calcium channel blocker” covers a heterogeneous class of compounds. The potentially harmful effects of some of the members of this family (i.e., reflex tachycardia, neurohormonal activation, negative inotropy, excessive hypotension) are not observed with all compounds and may even substantially differ between two formulations of the same compound (i.e., immediate release vs. sustained release) [1].
Recently, the new benzimidazolyl-substituted teraline derivative mibefradil (Ro 40-5967) has been shown [8, 9]to selectively inhibit in vitro the T-type calcium channels at concentrations that only partially blocked L-type currents. In early clinical trials and at plasma concentrations comparable to those used in the in vitro studies [9], mibefradil was well tolerated and exhibited both antianginal and antihypertensive properties [10, 11]. However, little is known about the cardiac effects of blocking the transient, low voltage-activated T-type calcium channel in humans. This study therefore sought to assess the effects of mibefradil on myocardial performance and systemic hemodynamic variables not only in patients with relatively normal cardiac function, but also in those with congestive heart failure and severe systolic dysfunction because this subgroup is particularly sensitive to the depressant effects of calcium entry blockade [3, 4].
1 Methods
Protocol overview. The present study was a two-center, open label, ascending-dose trial in which the safety and acute hemodynamic and cardiac effects of an intravenous infusion of mibefradil were assessed in patients with coronary artery disease and preserved (ejection fraction [EF] ≥40%) or depressed (EF <40%) systolic function. Two infusion regimens were used to reproduce the plasma concentrations observed at peak levels after long-term oral administration of 50 or 100 mg of mibefradil. Dose 1 (target concentration 400 ng/ml) consisted of a 15-min loading infusion at 1 mg/min followed by a maintenance infusion at 0.42 mg/min until the last measurements were completed. Dose 2 (target concentration 800 ng/ml) consisted of a 15-min loading infusion at 2.33 mg/min followed by a maintenance infusion at 0.75 mg/min. The total volume of fluid infused ranged from 120 ml after dose 1 to 220 ml after dose 2. The hemodynamic and neurohormonal measurements were obtained before and 30 min after the start of the loading infusion.
Patients. A total of 50 patients scheduled for diagnostic cardiac catheterization and stratified according to EF (≥40%, range 41% to 74%, n = 26; <40%, range 13% to 39%, n = 24) and the presence (n = 15, New York Heart Association functional class II or III) or absence (n = 35, functional class I) of clinical signs of congestive heart failure were included in the study. There were 45 male and 5 female patients with a mean age of 59 years (range 35 to 73), and there was no significant difference in demographic variables between dose groups. The patients fulfilling the selection criteria (see later) were assigned to treatment with mibefradil in a stepwise fashion for safety reasons. Thus, patients with a depressed EF and heart failure received doses 1 and 2 of mibefradil only when these regimens had been shown to be safe in the other patients.
Eligibility criteria. To be eligible, the patients were required to 1) be in sinus rhythm; 2) have significant coronary artery disease (defined as stenosis ≥60% of at least one major coronary vessel or evidence of a previous myocardial infarction at least 1 month before the study); and 3) meet the EF and functional class criteria at each step. Patients with unstable angina, a recent myocardial infarction, atrioventricular block of any degree, significant valvular or nonischemic myocardial disease as well with any significant noncardiac disease were excluded. All cardioactive drugs were discontinued at least 2 days before the study, except for angiotensin-converting enzyme inhibitors and short-acting nitrates, which were allowed up to 12 and 2 h before the study, respectively. All patients gave written informed consent to participate, and the study protocol was approved by the ethics committee at each participating center.
Data recording and analysis.Hemodynamic and angiographic study. Left heart catheterization was performed as described in detail previously [12]using an 8F pigtail catheter with a high fidelity micromanometer (Millar Instruments). Left ventriculography together with the electrocardiographic and pressure signals were digitized on-line (DVI Philips, 50 frames/s) and processed off-line (APU Philips, Philips Electronic Instruments). Ventricular silhouettes were digitized frame by frame on a video screen after mask substraction; the computer system derived the correction factor for X-ray magnification and calculated volumes every 20 ms by applying Simpson's rule. Wall thickness at the left ventricular (LV) equator was traced on the last unmasked diastolic frame and was computed for subsequent frames assuming a constant LV mass. Midwall circumferential stress was calculated with the formula of Mirsky [13]. Mean systolic wall stress was obtained by averaging data from the start to the end of ejection and the mean diastolic wall stress obtained by averaging data from the start of diastolic filling to end-diastole. Volume data were normalized using body surface area, and pressure-volume loops were plotted for each patient. Peak filling rate was calculated using a data smoothing program [14], and the angiographic cardiac index was calculated as


Plasma norepinephrine and plasma renin activity. Blood samples for plasma norepinephrine levels, plasma renin activity and mibefradil concentrations were obtained at baseline, before contrast material injection and after 30 min of infusion, before the second set of angiographic measurements. Blood samples were immediately chilled and centrifuged, and the plasma samples were stored at −80°C until assay as described previously [16]. Plasma norepinephrine levels were determined by a radioenzymatic assay using the enzyme catechol-o-methyl transferase [16]. Plasma renin activity was measured by the method described by Sealy and Laragh [17]. Plasma mibefradil concentrations were determined by high performance liquid chromatography with fluorescence detection.
Statistical analysis. Because the primary objective of this open study was safety, and because it did not include a placebo-controlled group, each group was analyzed separately, and the p values presented (two-tailed, based on paired t test calculations) are considered explorative. To account for multiple comparisons, the two-tailed t test in each of the four groups was performed only if a global test showed a statistically significant change from baseline for the selected variables regardless of a selected group. This global test was performed using an analysis of variance with the change from baseline as the dependent variable, a class variable describing the four groups as the independent variable and excluding the intercept variable from the model. In addition, the individual data were reviewed to detect any outlier in whom the hemodynamic response could be considered unfavorable (i.e., decrease in ejection fraction and increase in end-systolic volume, increase in LV end-diastolic pressure, excessive decrease in arterial pressure or heart rate). The linear relation between EF and end-systolic wall stress was derived using standard linear regression techniques.
2 Results
The mibefradil infusion was well tolerated in all subjects, and no serious adverse events were observed during the study. The baseline hemodynamic and LV function indexes together with the changes observed after mibefradil administration are summarized in Table 1Table 2.
| Variable | Dose 1 | Dose 2 | ||||||
|---|---|---|---|---|---|---|---|---|
| Baseline | Change From Baseline | Baseline | Change From Baseline | |||||
| No. of Pts | Mean ± SD | No. of Pts | Mean ± SD | No. of Pts | Mean ± SD | No. of Pts | Mean ± SD | |
| SAoP (mm Hg) | 12 | 145 ± 14 | 12 | −4.25 ± 8.96 | 13 | 161 ± 25 | 13 | −11.54 ± 10.32* |
| DAoP (mm Hg) | 11 | 75 ± 6 | 11 | −2.73 ± 6.18 | 13 | 76 ± 14 | 13 | −5.85 ± 3.83* |
| MAoP (mm Hg) | 11 | 102 ± 8 | 11 | −2.27 ± 7.96 | 13 | 108 ± 15 | 13 | −8.54 ± 5.83* |
| HR (beats/min) | 13 | 65 ± 8 | 13 | −3.46 ± 3.20* | 13 | 70 ± 10 | 13 | −0.92 ± 5.35 |
| LVSP (mm Hg) | 13 | 120 ± 22 | 13 | −6.00 ± 6.34* | 13 | 150 ± 13 | 13 | −6.69 ± 3.38* |
| LVEDP (mm Hg) | 13 | 18.7 ± 5.7 | 13 | 0.68 ± 3.89 | 13 | 20.2 ± 5.3 | 13 | 1.88 ± 3.45 |
| Peak + dP/dt (mm Hg/s) | 13 | 1,446 ± 216 | 13 | −31.15 ± 91.58 | 13 | 1,480 ± 304 | 13 | 44.54 ± 107.89 |
| Peak −dP/dt (mm Hg/s) | 13 | −1,728 ± 359 | 13 | 95.38 ± 153.72† | 13 | −1,836 ± 356 | 13 | 65.00 ± 152.90 |
| (dP/dt)/DP40 (1/s) | 13 | 23.7 ± 4.3 | 13 | −1.16 ± 2.64 | 13 | 23.0 ± 4.7 | 13 | 0.08 ± 2.08 |
| Tau (ms) | 13 | 49 ± 9 | 13 | 5.08 ± 4.80* | 13 | 48 ± 8 | 13 | 2.00 ± 5.26 |
| CI (liters/min per m2) | 13 | 3.2 ± 0.6 | 13 | −0.05 ± 0.52 | 13 | 3.8 ± 0.4 | 13 | 0.21 ± 0.42 |
| SVI (ml/m2) | 13 | 51 ± 11 | 13 | 1.00 ± 10.15 | 13 | 55 ± 7 | 13 | 4.85 ± 4.96 |
| LVESVI (ml/m2) | 13 | 50 ± 17 | 13 | 0.38 ± 6.09 | 13 | 54 ± 12 | 13 | −5.92 ± 6.86* |
| LVEDVI (ml/m2) | 13 | 103 ± 22 | 13 | 1.92 ± 12.49 | 13 | 112 ± 17 | 13 | 0.15 ± 6.44 |
| EF (%) | 13 | 52 ± 9 | 13 | 0.69 ± 5.81 | 13 | 52 ± 6 | 13 | 6.46 ± 6.95* |
| PER (ml/s) | 13 | −569 ± 130 | 13 | −4.54 ± 152.02 | 13 | −642 ± 133 | 13 | −116.5 ± 187.01† |
| PFR (ml/s) | 13 | 554 ± 205 | 13 | 5.77 ± 135.37 | 13 | 636 ± 124 | 13 | 88.77 ± 222.49 |
| Time to PFR (ms) | 13 | 218 ± 82 | 13 | 1.54 ± 51.94 | 13 | 229 ± 27 | 13 | 3.08 ± 35.45 |
| Mean VCF (circ/s) | 13 | 0.88 ± 0.23 | 13 | −0.02 ± 0.15 | 13 | 0.84 ± 0.17 | 13 | 0.10 ± 0.19 |
| MSWS (kdynes/cm2) | 13 | 261 ± 56 | 13 | 6.23 ± 45.43 | 13 | 275 ± 52 | 13 | −27.08 ± 31.78* |
| ESWS (kdynes/cm2) | 13 | 154 ± 53 | 13 | 2.46 ± 30.31 | 13 | 163 ± 45 | 13 | −26.69 ± 42.78† |
| MDWS (kdynes/cm2) | 13 | 34 ± 11 | 13 | 1.38 ± 7.12 | 13 | 45 ± 15 | 13 | −2.62 ± 13.30 |
| SWI (g/m2) | 11 | 56 ± 15 | 11 | −1.40 ± 8.69 | 13 | 61 ± 10 | 13 | −2.44 ± 5.64 |
| SVR (kdynes·s·cm−5) | 11 | 1,407 ± 341 | 11 | −36.36 ± 296.51 | 13 | 1,178 ± 200 | 13 | −146.5 ± 157.39† |
| Variable | Dose 1 | Dose 2 | ||||||
|---|---|---|---|---|---|---|---|---|
| Baseline | Change From Baseline | Baseline | Change From Baseline | |||||
| No. of Pts | Mean ± SD | No. of Pts | Mean ± SD | No. of Pts | Mean ± SD | No. of Pts | Mean ± SD | |
| SAoP (mm Hg) | 12 | 156 ± 30 | 12 | −8.92 ± 9.61* | 12 | 142 ± 19 | 12 | −11.50 ± 15.01† |
| DAoP (mm Hg) | 12 | 79 ± 12 | 12 | −8.17 ± 6.45* | 12 | 79 ± 15 | 12 | −12.17 ± 6.89* |
| MAoP (mm Hg) | 12 | 108 ± 18 | 12 | −9.00 ± 7.69* | 12 | 104 ± 14 | 12 | −12.67 ± 8.46* |
| HR (beats/min) | 12 | 72 ± 12 | 12 | −4.67 ± 5.43† | 12 | 81 ± 10 | 12 | −5.33 ± 7.04† |
| LVSP (mm Hg) | 12 | 141 ± 32 | 12 | −1.67 ± 9.72 | 12 | 141 ± 18 | 12 | −9.42 ± 9.39* |
| LVEDP (mm Hg) | 12 | 22.6 ± 6.4 | 12 | 0.95 ± 4.15 | 12 | 27.4 ± 6.2 | 12 | 0.29 ± 3.05 |
| Peak + dP/dt (mm Hg/s) | 12 | 1,333 ± 391 | 12 | −8.08 ± 164.34 | 12 | 1,387 ± 354 | 12 | −130.2 ± 112.33* |
| Peak −dP/dt (mm Hg/s) | 12 | −1,319 ± 296 | 12 | −5.92 ± 95.40 | 12 | −1,364 ± 309 | 12 | 95.42 ± 94.46* |
| (dP/dt)DP40 (1/s) | 12 | 19.7 ± 5.5 | 12 | −0.32 ± 1.86 | 12 | 18.9 ± 5.0 | 12 | −1.88 ± 1.18† |
| Tau (ms) | 12 | 60 ± 9 | 12 | 2.25 ± 4.05 | 12 | 54 ± 10 | 12 | 4.50 ± 5.14† |
| CI (liters/min per m2) | 12 | 3.3 ± 1.0 | 12 | −0.12 ± 0.65 | 12 | 3.6 ± 0.4 | 12 | −0.00 ± 0.48 |
| SVI (ml/m2) | 12 | 47 ± 12 | 12 | 2.00 ± 6.34 | 12 | 44 ± 10 | 12 | 3.75 ± 7.90 |
| LVESVI (ml/m2) | 12 | 112 ± 52 | 12 | −7.67 ± 8.15* | 12 | 130 ± 45 | 12 | −4.33 ± 9.09 |
| LVEDVI (ml/m2) | 12 | 154 ± 55 | 12 | 0.00 ± 7.71 | 12 | 170 ± 49 | 12 | 2.17 ± 7.42 |
| EF (%) | 12 | 29 ± 8 | 12 | 5.00 ± 5.06* | 12 | 24 ± 8 | 12 | 4.50 ± 5.20† |
| PER (ml/s) | 12 | −479 ± 147 | 12 | −50.75 ± 113.74 | 12 | −454 ± 112 | 12 | −45.00 ± 122.56 |
| PFR (ml/s) | 12 | 487 ± 147 | 12 | 0.67 ± 148.56 | 12 | 514 ± 139 | 12 | −5.67 ± 187.26 |
| Time to PFR (ms) | 12 | 285 ± 91 | 12 | −5.00 ± 80.06 | 12 | 268 ± 121 | 12 | 11.67 ± 55.57 |
| Mean VCF (circ/s) | 12 | 0.42 ± 0.15 | 12 | −0.10 ± 0.13† | 12 | 0.36 ± 0.16 | 12 | 0.12 ± 0.15† |
| MSWS (kdynes/cm2) | 12 | 316 ± 90 | 12 | −10.58 ± 39.54 | 12 | 308 ± 40 | 12 | −42.17 ± 32.84* |
| ESWS (kdynes/cm2) | 12 | 269 ± 65 | 12 | −41.58 ± 39.28* | 12 | 261 ± 43 | 12 | −40.42 ± 42.85* |
| MDWS (kdynes/cm2) | 12 | 74 ± 30 | 12 | −15.17 ± 13.35* | 12 | 91 ± 18 | 12 | −14.67 ± 15.84* |
| SWI (g/m2) | 12 | 51 ± 19 | 12 | −3.67 ± 8.80 | 12 | 41 ± 10 | 12 | −4.03 ± 8.56 |
| SVR (kdynes·s·cm−5) | 12 | 1,513 ± 484 | 12 | −93.08 ± 255.57 | 12 | 1,266 ± 232 | 12 | −162.2 ± 206.66† |
Effects of mibefradil in patients with preserved systolic function. In this group of patients, the plasma levels reached after doses 1 and 2 were 446 ± 66 ng/ml (range 323 to 532, n = 13) and 898 ± 196 (range 659 to 1281, n = 13), respectively. No clinically significant changes in hemodynamic or LV function indexes were evident after dose 1 in this subset of patients. However, dose 2 induced a modest but statistically significant vasodilation, as reflected by a 12% decrease in systemic vascular resistance and by a 8.5-mm Hg decrease in mean aortic pressure (both p < 0.01). This decrease in systemic impedance resulted in a reduced LV afterload (−16% in end-systolic wall stress, p < 0.05), and mean LV EF improved from 52% to 58% (p < 0.01). Heart rate tended to decrease, but cardiac index and the isovolumic indexes of relaxation and inotropic state were unchanged. The changes in plasma norepinephrine and plasma renin activity were also insignificant (Table 3).
| Dose 1 | Dose 2 | |||
|---|---|---|---|---|
| Baseline (mean ± SD) | Change From Baseline (mean ± SD) | Baseline (mean ± SD) | Change From Baseline (mean ± SD) | |
| Norepinephrine (ng/ml) | ||||
| EF >40% (n = 13) | 325.85 ± 91.68 | 45.62 ± 131.74 | 308.00 ± 92.38 | 91.92 ± 82.37 |
| EF <40% (n = 12) | 290.42 ± 151.26 | 43.33 ± 56.47 | 320.08 ± 164.52 | 78.83 ± 128.26 |
| Plasma renin activity (ng/ml per h) | ||||
| EF >40% (n = 13) | 0.73 ± 0.54 | 0.02 ± 0.18 | 0.72 ± 0.51 | −0.07 ± 0.18 |
| EF <40% (n = 12) | 0.68 ± 0.65 | −0.20 ± 0.40 | 0.72 ± 0.71 | −0.05 ± 0.26 |
Effects of mibefradil in patients with depressed systolic function. In this study group, the plasma levels reached after doses 1 and 2 were 559 ± 238 ng/ml (range 250 to 1165) and 1,052 ± 284 ng/ml (range 688 to 1532), that is, ∼30% to 40% higher than predicted and higher than in patients with preserved LV function. In this subset, both doses induced a significant reduction in heart rate, mean aortic pressure and end-systolic wall stress, with an improvement in EF (+5.0% after dose 1 and +4.5% after dose 2 [Table 2]). Left ventricular end-diastolic pressure was unchanged, but mean diastolic wall stress decreased with both the doses. Analysis of the pressure-volume data suggests that this decrease was related to a downward shift in the pressure-volume loop that occurred during diastole in 70% of patients without congestive heart failure (CHF) and in 9 of 12 patients with CHF and a low EF. The other indexes of diastolic function, such as peak filling rate and time to peak filling, were unchanged, and the index of isovolumetric relaxation tau was prolonged. Whereas the angiographic cardiac index was unchanged at both doses levels, the indexes of inotropic state and relaxation became slightly but significantly depressed after the administration of dose 2 of mibefradil. However, all these indexes are heart rate, preload and afterload dependent, and examination of the LV and aortic pressure tracings revealed that in many of these patients, neither peak positive dP/dt nor (dP/dt) DP40 remained isovolumetric during mibefradil infusion (i.e., dP/dt had to be measured at a mean developed pressure of 68 mm Hg, whereas the mean arterial diastolic pressure was 66 mm Hg), which reduces the value of these indexes to detect true changes in inotropic state.
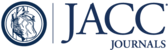
Therefore, to better characterize the effects of mibefradil on cardiac inotropy, the relation between EF and end-systolic wall stress and the individual pressure-volume loops was examined. Fig. 1 illustrates the inverse relations between end-systolic wall stress and EF at baseline and during mibefradil infusion. There were no statistically significant differences in the slope of these two relations. Furthermore, individual data points after mibefradil were still within the 95% confidence intervals of baseline relations. At the group level, these findings indicate no significant difference in myocardial performance before and after the short-term infusion of mibefradil.

Relation between end-systolic wall stress and EF before and after mibefradil administration. No significant difference in slope was noted after drug administration. Open symbols = patients with EF <40% at baseline; solid symbols = patients with EF >40% at baseline; dashed lines = 95% confidence intervals.
Analysis of the individual pressure-volume loops indicated that in all but four patients, the decrease in systolic pressure was accompanied by a decrease in end-systolic volume. Nevertheless, after dose 1, and despite a decrease in peak systolic and end-systolic pressures, one patient with CHF (Patient 12) had an unchanged end-systolic volume (Fig. 2), whereas another patient with a low EF but no CHF (not illustrated) had an increase in end-systolic volume. Furthermore, after dose 2, end-systolic volume was clearly increased after mibefradil despite a reduction in end-systolic pressure in two patients with CHF (Patients 36 and 39) (Fig. 3). Such an abrupt rightward shift observed in three patients can only be explained in terms of cardiac mechanics by a negative inotropic effect. No such shift was noted after doses 1 or 2 in patients with a preserved EF. Finally, no statistically significant changes in plasma norepinephrine levels or plasma renin activity were detected at the group level (Table 3).

Individual pressure-volume loops in six patients (Pat.) with EF <40% and CHF before (open circles) and after (solid circles) administration of mibefradil (dose 1). End-systolic volume decreased in all but one patient (Patient 12), and there was a downward shift of the diastolic pressure-volume data in four patients.

Individual pressure-volume loops in six patients (Pat.) with EF <40% and CHF before (open circles) and after (solid circles) administration of mibefradil (dose 2). End-systolic volume increased substantially despite reduced systolic pressure in two patients (Patients 36 and 39), suggesting negative inotropy. The diastolic pressure-volume data were shifted downward (improved distensibility) in five patients.
3 Discussion
The present study sought to assess the safety of short-term administration of the calcium channel blocker mibefradil. Calcium antagonists have been implicated in various adverse effects, including aggravation of myocardial ischemia and CHF [1–4]. Among the mechanisms believed to underlie these harmful effects are reflex tachycardia, reflex neurohormonal activation, negative inotropic action and excessive hypotension. Special attention was therefore directed toward these pharmacodynamic effects of mibefradil.
Effects on heart rate and neurohormones. The data indicated that intravenous mibefradil, at doses used in the study, primarily acted as a mild arteriodilator with a relatively flat dose-response relation and was tolerated well by the patients. Of interest was the finding that the drug did not trigger reflex tachycardia; rather, a slight bradycardia was generally produced, particularly in patients with a rest heart rate >70 beats/min. This observation is in agreement with early clinical studies using oral mibefradil [10, 11, 18]. The bradycardic action of mibefradil is most likely related to the selective inhibition of the T-type calcium channels that are predominant in pacemaker cells of the sinoatrial node [19]as well as in smooth muscle cells with pacemaker function [20]. It is also noteworthy that no significant increases in plasma norepinephrine levels were detected at the group level, even when data from all patients were pooled. In fact, 27 patients had increases or decreases well within the limits of the analytical methods used. Twenty-three patients had an increase >15% of baseline values. Thus, although some degree of sympathetic activation may have been present in some patients, the magnitude of the changes in plasma norepinephrine levels was much less than that after intravenous dihydropyridine administration [21], and a strong reflex sympathetic activation is unlikely to have masked a drug-induced myocardial depression. There was also no effect on plasma renin activity, but in this case the effects of the contrast material on the juxtaglomerular apparatus may have contributed to blunt the response [12].
Effects on inotropic state. The direct effects of calcium channel blockers on LV inotropic state are notoriously difficult to assess in the clinical setting. Using the classical indexes of inotropic state and relaxation, no significant direct effects of mibefradil on myocardial performance could be detected in patients with a preserved LV systolic function. In patients with a low EF, however, examination of the pressure-volume loops yielded some evidence of depressed myocardial function in three patients (one without and two with CHF). In the absence of a placebo group, it could be argued that such changes could not be entirely drug related and might also reflect the impact of the angiographic procedures. Moreover, it is noteworthy that despite supratherapeutic concentrations, no patient experienced clinically significant hemodynamic deterioration, as has been described after nifedipine [22]. Nevertheless, that these three patients were clustered in the subgroup with a low EF, and the most obvious depression of myocardial function occurred after the highest dose in two of these patients, suggests that this was a real pharmacologic effect. This hypothesis is also supported by the finding that the time constant of isovolumic relaxation was significantly prolonged in this subgroup after dose 2 despite the decrease in blood pressure and minimal changes in heart rate. Patients with heart failure are known to have alterations in the excitation-contraction-relaxation coupling [23]and to be more sensitive to L-channel blockade [3, 4, 24]. At the highest plasma levels observed with dose 2 in the heart failure subset, the changes in relaxation observed are therefore compatible with L-channel blockade inducing some degree of myocardial depression. To place this observation into correct clinical perspective, it is important to recall that the plasma levels measured in patients with a depressed EF were 30% to 40% higher than predicted and higher than those generally required to produce a therapeutic benefit [10]. This pharmacokinetic difference was accompanied by pharmacodynamic consequences: The decreases in mean arterial pressure were indeed of the same magnitude after dose 1 in patients with a low EF (−9.0 mm Hg) as those after dose 2 (−8.5 mm Hg) in patients with a preserved EF. If similar pharmacokinetic differences are present after oral administration, this presence suggests that the dose of mibefradil should be reduced in patients with poor LV function or CHF, or both.
Conclusions. Intravenous mibefradil was well tolerated. The overall pharmacodynamic profile (bradycardia, decreased systolic wall stress, improved EF and minor sympathetic activation, if any, even after intravenous administration), coupled with evidence of antianginal [10, 25]and antihypertensive properties, warrants further study of this compound in a larger population. Recent data [26]obtained with amlodipine suggest that a subgroup of patients with CHF may benefit, in terms of survival, from calcium channel blocker therapy. Whether a similar or greater benefit can be provided by a relatively specific T-type calcium channel blocker is presently being investigated in a large-scale mortality trial. Until the results of this trial are available, caution should still be exerted with mibefradil in patients with CHF in light of the possibility of myocardial depression.
A.1 Abbreviations and Acronyms
CHF = congestive heart failure
dP/dt = first derivative of left ventricular pressure
(dP/dt)/DP40 = dP/dt measured at a developed pressure of 40 mm Hg
EF = ejection fraction
LV = left ventricular
1. Ruzicka M, Leenen FHH. Relevance of intermittent increases in sympathetic activity for adverse outcome on short-acting calcium antagonists. In: Laragh JH, Brenner BM, editors. Hypertension: Pathophysiology, Diagnosis and Management. New York: Raven Press, 1995:2815–25.
2. Furberg CD, Psaty BM, Meyer JV. Nifedipine: dose-related increase in mortality in patients with coronary heart disease. Circulation 1995;92:1326–31.
3. : "Pathophysiological mechanisms underlying the adverse effects of calcium channel-blocking drugs in patients with chronic heart failure". Circulation 1989; 80: 59.
4. Pouleur H. Calcium entry blockers in congestive heart failure and in asymptomatic left ventricular dysfunction. In: Barnett D, Pouleur H, Francis G, editors. Heart Failure. New York: Marcel Dekker, 1993:287–301.
5. Aursnes I, Litleskare I, Froyland H, Abdelnoor M. Association between various drugs used for hypertension and risk of acute myocardial infarction. Blood Pressure 1995;4:157–63.
6. Psaty BM, Heckbert SR, Koepsell TD, et al. The risk of myocardial infarction associated with antihypertensive drug therapies. JAMA 1995;274:620–5.
7. : "Long-term survival and use of antihypertensive medications in older persons". J Am Geriatr Soc 1995; 43: 1.
8. Mehrke G, Zong XG, Flockerzi V, Hofmann F. The Ca++-channel blocker Ro 40-5967 blocks differently T-type and L-type Ca++ channels. J Pharmacol Exp Ther 1994;271:1483–8.
9. Mishra SK, Hermsmeyer K. Selective inhibition of T-type Ca2+ channels by Ro 40-5967. Circ Res 1994;75:144–8.
10. : "Ro 40-5967: a new nondihydropyridine calcium antagonist". Cardiovasc Drug Rev 1991; 9: 4.
11. Portegies MCM, Schmitt R, Kraiij CJ, et al. Lack of negative inotropic effects of the new calcium antagonist Ro 40-5967 in patients with stable angina pectoris. J Cardiovasc Pharmacol 1991;18:746–51.
12. Rousseau MF, Gurné O, van Eyll C, Benedict CR, Pouleur H. Effects of benazeprilat on left ventricular systolic and diastolic function and neurohumoral status in patients with ischemic heart disease. Circulation 1990;81 Suppl III:III-123–9.
13. Mirsky I. Elastic properties of the myocardium: a quantitative approach with physiological and clinical applications. In: Berne RM, Sperelakis N, editors. Handbook of Physiology, Section 2: The Cardiovascular System. Baltimore: Williams & Wilkins, 1979:497–531.
14. van Eyll C, Pouleur H, Charlier AA, Brasseur LA, Gurné O, Rousseau MF. Interest of quantitative diastolic regional wall motion analysis in ischemic heart disease. In: Computers in Cardiology. Salt Lake City: IEEE Computer Society, 1984:219–22.
15. Braunwald E, Ross J Jr, Sonnenblick EH. Methods for assessing cardiac contractility. In: Braunwald E, Ross J Jr, Sonnenblick EH, editors. Mechanisms of Contraction of the Normal and Failing Heart. Boston: Little Brown, 1976:130–65.
16. Hussain MN, Benedict CR. Radioenzymatic microassay for simultaneous estimations of dopamine, norepinephrine, and epinephrine in plasma, urine and tissues. Clin Chem 1985;31:1861–4.
17. Sealy J, Laragh JH. How to do plasma renin assay. In: Laragh JH, editor. Topics in Hypertension. New York, York Medical Books, 1980:244–56.
18. Muntinga HJ, van der Vring JAFM, Niemeyer MG, et al. Effect of mibefradil on left ventricular diastolic function in patients with congestive heart failure. J Cardiovasc Pharmacol 1996;27:652–6.
19. Bean BP. Classes of calcium channels in vertebrate cells. Annu Rev Physiol 1989;51:367–84.
20. Hermsmeyer K. Differences of calcium channels in vascular muscle in hypertension. Am J Hypertens 1991;4:412–5.
21. Rousseau MF, Vincent MF, Van Hoof F, Van den Berghe G, Charlier AA, Pouleur H. Effects of nicardipine and nisoldipine on myocardial metabolism, coronary blood flow and oxygen supply in angina pectoris. Am J Cardiol 1984;54:1189–94.
22. Packer M, Lee WH, Medina N, Yushak M, Berstein JL, Kessler PD. Prognostic importance of the immediate hemodynamic response to nifedipine in patients with severe left ventricular dysfunction. J Am Coll Cardiol 1987;10:1303–11.
23. Feldman MD, Copelas L, Gwathmey JK, Phillips P, Warren SE, Schoen FJ. Deficient production of cyclic AMP: pharmacologic evidence of an important cause of contractile dysfunction in patients with end-stage heart failure. Circulation 1987;75:331–9.
24. : "Calcium-channel blockade in the management of severe congestive heart failure: a bridge too far". Circulation 1987; 75: 56.
25. Braun S, van der Wall EE, Emanuelsson H, Kobrin I, on behalf of the Mibefradil International Study Group. Effects of a new calcium antagonist, mibefradil (Ro 40-5967), on silent ischemia in patients with stable chronic angina pectoris: a multicenter placebo-controlled study. J Am Coll Cardiol 1996;27:317–22.
26. : "for the PRAISE Investigators. Safety of amlodipine in severe heart failure: reduction of sudden death in non-ischemic heart disease [abstract]". J Am Coll Cardiol 1996; 27: 281A.
{kind=link}
{kind=link}
{kind=link}