

Noninvasive Screening for Coronary Atherosclerosis and Silent Ischemia in Asymptomatic Type 2 Diabetic Patients: Is it Appropriate and Cost-Effective?
Viewpoint and Commentary
Coronary artery disease (CAD) accounts for 65% to 80% of deaths in diabetic patients. The merits of screening asymptomatic type 2 diabetic patients for either (A) the presence of coronary atherosclerosis by imaging of coronary calcification using cardiac computed tomography or (B) silent ischemia by stress myocardial perfusion imaging (MPI) remain controversial. Some observers have advocated for such noninvasive screening in at least the subset of the diabetic population who have significant clinical CAD risk factors, so that the highest risk patients for future cardiac events can be identified and offered more aggressive intensive medical therapy or coronary revascularization and optimum medical therapy. Computed tomography coronary calcium scanning could be the first noninvasive screening test in these clinically high-risk diabetic patients, followed by stress MPI to detect silent ischemia in those who exhibit high coronary calcium scores.
Introduction
Considerable discussion and debate are ongoing regarding the value of noninvasive screening for noncritical coronary atherosclerosis or silent ischemia secondary to flow-limiting stenoses in asymptomatic type 2 diabetic patients. This controversy about the merits of noninvasive screening for coronary artery disease (CAD) in asymptomatic diabetic patients has arisen for a number of reasons. Coronary artery disease accounts for 65% to 80% of deaths (1) in diabetic patients, and in 2007 approximately 17 million Americans have diabetes. By 2050, this number could increase to 48 million (2). Women with type 2 diabetes are particularly prone to cardiovascular disease and its complications. In one study, the hazard ratio for cardiovascular mortality for women with both metabolic syndrome and diabetes was approximately 9.5, compared with women without diabetes or metabolic syndrome (3). The age-adjusted risk of CAD in diabetic women, compared with nondiabetic women, is 5.1, whereas in men this value is 2.4 (4). The actual prevalence of significant coronary atherosclerosis in a truly representative population of type 2 diabetic patients has not been ascertained. One estimate is that 20% of diabetic patients have established CAD (5). In an asymptomatic and uncomplicated cohort of type 2 diabetic patients, 46.3% had evidence of coronary calcification indicative of coronary atherosclerosis (6). In an autopsy study of diabetic patients, the prevalence of anatomic CAD was 50% to 81% (7).
Diabetic patients with inducible ischemia on stress myocardial perfusion imaging, using single-photon emission computed tomography (SPECT), have a significantly higher subsequent annual cardiac death or myocardial infarction rate than nondiabetic patients with ischemia (10% vs. 6%) (8). In this pooled analysis of studies in the literature, female diabetic patients with an abnormal SPECT study had an annual rate of approximately 11.5% for cardiac death/myocardial infarction, compared with just above 6% for men. In one study of female diabetic patients with a high-risk stress SPECT perfusion scan, characterized by a multivessel disease pattern, only 60% survived, without infarction, in the ensuing 3 years. For the male diabetic patients with a high-risk scan, this value was 79% (9). Similarly, diabetic patients with an abnormal ischemic stress echocardiographic response have a worse prognosis than nondiabetic patients with stress-induced ischemia (10). The true prevalence of silent ischemia using noninvasive stress imaging in asymptomatic type 2 diabetic patients is not known, but ranges from 16% to 59% have been reported (11–15), depending on the pretest clinical risk profile of the patient groups studied. The DIAD (Detection of Ischemia in Asymptomatic Diabetics) study (14) comprised a lower-risk group of type 2 diabetic patients than those imaged in the other studies. For example, diabetic patients with an abnormal resting electrocardiogram (ECG) were not enrolled in the DIAD study. Fifty percent of patients in the Mayo Clinic cohort were referred for preoperative risk assessment, and 43% had ECG Q waves while 28% had peripheral vascular disease (12). Female diabetic patients with normal perfusion scans or normal stress echocardiograms still have an annual hard cardiac event rate of ≥3.0% (8,10). In one observational database, diabetic patients with ischemia had a better survival rate with revascularization rather than with medical therapy (16).
Diabetic patients with coronary atherosclerosis as determined by computed tomography (CT) calcium scanning have a worse outcome with respect to cardiac death and nonfatal infarction than nondiabetic patients with the same coronary artery calcium (CAC) score (17). Interestingly, compared with nondiabetic patients, diabetic patients with a zero CAC score had a similar annual mortality rate of 0.36%. One group found that 48% of diabetic patients had a CAC score compatible with significant CAD (18). In asymptomatic diabetic patients, the prevalence of stress-induced ischemia increases the higher the CAC score is on CT scanning (6). In that study, 23% of asymptomatic diabetic patients with a CAC of 101 to 400 had a positive stress SPECT scan. Those with CAC >400 had a 48% prevalence of silent ischemia, and this number increased to 71.4% for the asymptomatic diabetic patients with a CAC of >1,000. The greater the extent of ischemia, the worse the clinical outcome, and the CAC score was superior to established risk factors for predicting silent ischemia and cardiac events (6). The prevalence of silent ischemia for any given CAC score range was higher in this study than in 2 prior reports (19,20). Conversely, in the study by Anand et al. (6), all diabetic patients with a CAC score between 0 and 10 had normal SPECT studies and excellent prognoses.
Some thought leaders have recommended the adoption of decision-making algorithms that advocate noninvasive screening for CAD in the asymptomatic diabetic population, and some have suggested that screening at least some subset of the diabetic population may be clinically valuable (21–24). These ideas are supported by the high prevalence of CAD and high cardiovascular mortality rate in the diabetic population, the substantial risk of future cardiac events in asymptomatic diabetic patients with subclinical atherosclerosis (as assessed by CT calcium scanning), the prevalence of silent ischemia in diabetic patients, and the higher cardiac event rate with inducible ischemia for diabetic patients versus nondiabetic patients. Other experts, however, remain skeptical or cautious regarding the worth and cost-effectiveness of screening diabetic patients for coronary atherosclerosis or silent ischemia (25,26). Some observers are open to the concept of screening asymptomatic diabetic patients but want to see a randomized clinical trial of screening versus no screening to establish efficacy, recognizing that the cost of such a trial would be enormous and could only be funded by a governmental agency (27).
Certainly, diabetic patients with symptoms such as chest pain or dyspnea are presently being evaluated appropriately with noninvasive and/or invasive strategies, depending upon their clinical presentation. In one combined report from Cedars Sinai, Los Angeles, and the Basel groups, 51% of 151 diabetic patients with dyspnea and no chest pain had objective evidence of CAD by SPECT criteria (13). Asymptomatic diabetic patients are already being treated as CAD equivalents with respect to guidelines for lipid lowering (low-density lipoprotein [LDL] cholesterol <100 mg/dl). In diabetic patients with established CAD, LDL cholesterol levels should be lowered to below 70 mg/dl (28).
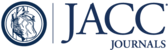
In this issue of the Journal, Diamond et al. (29) analyze the expected costs and benefits associated with routine screening of asymptomatic diabetic patients for subclinical atherosclerotic disease, using myocardial perfusion imaging. They discuss the merits of a conditional test-treatment strategy in which scintigraphic testing is followed by statin treatment in positive test responders, compared with an unconditional treatment strategy involving no testing, but rather treating all diabetic patients with statins. Their analysis shows that unconditional treatment costs 24% less and prevents 25% more atherosclerotic events annually. This essay was written primarily in response to the review by Bax et al. (22) representing a group of physicians from Europe and the U.S. identified as the “Global Dialogue Group for Evaluation of Cardiovascular Risk in Patients With Diabetes.” Bax et al. (22) reviewed all the data in the literature pertaining to screening asymptomatic diabetic patients for silent ischemia. The evidence they cited suggested a “potential algorithm,” summarized in Figure 1.Asymptomatic diabetic patients over 40 years old, who are classified as moderate or high risk based on a conventional risk evaluation, are referred to stress myocardial perfusion imaging. Those with moderate or severe perfusion abnormalities would undergo invasive coronary angiography. Those with mild defects would be candidates for aggressive risk factor modification and medical therapy, with possible repeat testing in 2 years. Diabetic patients with normal perfusion scans would have their risk factors modified according to practice guidelines and undergo “conventional” follow-up. Recall that diabetic patients with normal SPECT studies, particularly women, still have an approximate 2.5% to 3.0% annual hard event rate in follow-up. Later in their review, Bax et al. (22) then modify this “potential algorithm” in light of the previously discussed study by Anand et al. (24), which used CAC scoring by CT to identify which patients would benefit most from subsequent stress perfusion imaging. In this scenario, the algorithm in Figure 1would be modified to refer patients to stress perfusion imaging only after CT calcium scanning (a much less expensive procedure) revealed the presence of significant atherosclerosis. The cutoff CAC scores for such triage to stress perfusion imaging is not yet clear, but could be >100 or >400, based on the results of ongoing clinical research in this area.

Algorithm for Risk Assessment and Management in Asymptomatic Type 2 Diabetic Patients
MPS = myocardial perfusion imaging. Reprinted with permission from Bax et al. (22).
Diamond et al. (29) reject the screening approaches described in the preceding text. Using what they call a “back-of-the-envelope” calculation, they conclude that an alternative unconditional strategy to noninvasive test screening, which they refer to as “test no one, and treat everyone,” yields better outcomes at lower cost. In the absence of treatment, 280,000 events per year are expected in a target population of 14 million diabetic patients (2% event rate). Using data from randomized trials, they assume that treating everyone will reduce events by 30%—84,000 events prevented at a treatment cost of $10.1 billion annually ($720 a year for statin therapy). The cost per prevented event is $120,238. Without going into the exact details of their methodology, the principle employed in the calculations for the test-treatment strategy is Pareto’s rule (30), which states that a test like myocardial perfusion imaging will identify approximately 20% of the population among whom 80% of the events will occur. By applying this principle to the population of 14 million diabetic patients, only 2.8 million are treated, which would prevent 67,200 events at a cost of $13.3 billion. The cost per prevented event is $197,917. Again, in this strategy, only the higher-risk population with a positive scan are treated (medically, with statins, in their model) with a subsequent reduction in events of only 30%. The authors’ calculations imply that the 11.2 million patients that had a negative test would not be treated. Another assumption in their testing strategy is that sensitivity and specificity of stress testing are both 80%. In actuality, sensitivity is closer to 85% to 90%, with near 90% specificity for gated SPECT and attenuation correction. Finally, the authors also go on to show that less expensive alternative screening tests like CAC scanning do no better than the unconditional “treat everyone” strategy. The specificity of CAC for coronary atherosclerosis is definitely higher than 80%.
Although hypothetical and based on certain assumptions with which some would not agree, the essay by Diamond et al. (29) is of great value in that it is provocative and highlights the limitations of our current knowledge base on the subject of the cost-effectiveness of screening asymptomatic type 2 diabetic patients. On one hand we know that type 2 diabetic patients, especially those with metabolic syndrome and multiple CAD risk factors, have a substantially increased risk of cardiac events compared with asymptomatic nondiabetic patients. We know that diabetic patients with ischemia have a worse outcome than nondiabetic patients with ischemia, with either medical therapy or revascularization. We also know that diabetic patients without flow limiting stenoses, but with subclinical atherosclerosis according to CAC scanning, have a higher event rate than nondiabetic patients with subcritical atherosclerotic lesions. On the other hand, we do not know, in a representative, unbiased, and nonselected population of type 2 diabetic patients, the true prevalence of silent ischemia or the true prevalence of significant subclinical coronary atherosclerosis, particularly the percentage of patients vulnerable to acute coronary events or sudden cardiac death (e.g., due to plaque rupture). The DIAD study showed a rather low prevalence of inducible ischemia and high-risk scans in asymptomatic type 2 diabetic patients (14), whereas the Mayo Clinic- and Cedars Sinai-based studies showed a much higher prevalence of patients with high-risk scans (11–13).
A problem with the approach favored by Diamond et al. (29) is that, in the conditional testing strategy, patients with a negative noninvasive study presumably are not treated with statins. This is not realistic, since our practice guidelines clearly state that all asymptomatic type 2 diabetic patients, regardless of the presence of subclinical CAD, should have their LDL cholesterol lowered to below 100 mg/dl. To accomplish this goal, a large percentage of patients require statin therapy. Thus, the question should not be whether noninvasive test screening is appropriate for identifying which diabetic patients should be treated with statins, but whether a very high-risk group of asymptomatic diabetic patients can be identified for whom very aggressive therapy (including LDL cholesterol lowered to <70 mg/dl), with or without revascularization, would be beneficial and cost-effective. Another potential limitation of their calculations is that they do not take into account the costs incurred by the crossover of patients in the nontested unconditionally treated group who develop symptoms or experience cardiac events that may have been prevented had they been initially tested. A high percentage of such crossover patients, who might have already had significant coronary atherosclerosis, would have been detected earlier in the noninvasive testing strategy and more aggressively managed, thereby possibly reducing the risk of future adverse cardiovascular events. Downstream costs for patients with positive scans in the testing arm are also not calculated. An unknown number of patients with positive test results would not just be treated aggressively with medical therapy, but would be referred for coronary angiography. A percentage of these patients would subsequently undergo coronary revascularization, which increases costs even more than estimated by Diamond et al. (29). Actually, upfront costs are only a small portion of the induced costs. Upfront costs according to Shaw and Iskandrian (8) are approximately 20% of the induced costs for a procedure.
Another question is whether the costs of screening and prevention reduce costs from further overt disease (31). For example, if CT calcium scanning is used as the first screening test, and patients with CAC scores of >400 are very aggressively managed, leading to a reduction in subsequent hospitalizations for acute coronary events, that represents a reduction in overall costs in the conditional test-treatment strategy population. A problem with this concept is that patients with predominantly soft plaques that are prone to rupture, causing an acute coronary event, are missed by CT scanning for coronary calcification. One study estimated that 16% of patients (10% were diabetic patients) with negative calcium scores had noncalcified plaques seen on CT angiography (32). Another issue to consider is whether revascularization is superior to medical therapy in asymptomatic diabetic patients with silent ischemia, particularly those with high-risk SPECT scans or stress echocardiograms. If it is not superior, what would be the value of a conditional test-treatment strategy? Such a strategy is predicated, in part, on the assumption that identifying such patients with silent ischemia improves their outcomes because of more aggressive treatment strategies than are applied to those with normal or low-risk results. We do not have any data from randomized clinical trials in which asymptomatic type 2 diabetic patients with ischemic noninvasive test findings were randomized to medical therapy versus revascularization and appropriate medical therapy to help us resolve this issue. Perhaps such information will be forthcoming when the BARI-2D (Bypass Angioplasty Revascularization Investigation in Type 2 Diabetics) trial results are eventually released. We do, however, have 1 nonrandomized study showing improved survival in asymptomatic diabetic patients with high-risk SPECT imaging results treated with coronary artery bypass grafting (33).
A compromise approach to the screening controversy should perhaps be entertained and then, if affordable, a clinical randomized trial performed to validate it. This approach involves an algorithm that confines noninvasive test screening to a specific high-risk population of asymptomatic type 2 diabetic patients. First, such a population of asymptomatic type 2 diabetic patients that truly represents a high-risk cohort by acknowledged epidemiologic data and results of prospective studies needs to be characterized, using clinical and routine laboratory variables. For example, it may be that patients with both type 2 diabetes and metabolic syndrome, associated with multiple CAD risk factors, who are over the age of 40 comprise this high-risk group. Women with this profile may be at a higher risk for future events than men. Certainly, asymptomatic type 2 diabetic patients with abnormal resting ECGs or peripheral arterial disease would fall into this high-risk category. This clinically high-risk population of patients would not only have the LDL target below 70 mg/dl, but would proceed to noninvasive testing with CT calcium scanning. Those with CAC scores of >400 would go on to stress perfusion imaging. If ≥10% of the left ventricle showed ischemia, they would go on to coronary angiography and undergo coronary revascularization, according to accepted angiographic criteria. For subcritical stenoses detected by angiography and not associated with ischemia on noninvasive testing, fractional flow reserve measurements might be obtained to better determine the functional significance of the demonstrated lesions. Those patients with abnormal scans with <10% ischemia would be treated with beta-blockers and other risk factor modification with repeat testing in perhaps 1 or 2 years. In this hypothetical algorithm, patients with normal scans would be monitored carefully for compliance with medications and continued risk factor modification as mentioned in the preceding text. If a randomized study were to be performed to validate this algorithm combining clinical risk stratification and noninvasive testing, it might be designed as an equivalence trial to identify whether the imaging strategy can equal the “test no one and treat all” strategy as characterized by Diamond et al. (29). The primary outcome is death or infarction. Secondary outcomes are quality of life (personal well-being and treatment satisfaction) and total cost, including downstream 5-year costs.
Eventually, we will need better imaging techniques that can assess both plaque burden (soft and calcified) and the extent of vulnerable plaques. These techniques will require molecular imaging, currently being tested in animal and patient models. These techniques permit delineation of plaque macrophage density and inflammatory markers (e.g., matrix metalloproteinases), the thickness of the fibrous cap, the extent of the lipid-laden necrotic core, fibrin deposition, and the presence of neovessels (34–36). If total plaque burden and some index of “vulnerability” could be detected noninvasively, at a reasonable cost, then this approach may be preferable to plaque CAC imaging, which is merely reflective of the presence of atherosclerosis. Soft plaques, as previously mentioned, are missed, and no information on vulnerability to rupture is obtained.
We are in an era in which the concept of screening asymptomatic subjects is being debated. There are sound arguments on both sides, but in the long run, the controversy can only be resolved by gathering evidence for or against screening, which requires data from a randomized clinical trial. The cost of such a trial would be enormous since, as Diamond et al. (29) speculate in their essay, to prove superiority of a testing strategy over a treat-all strategy using their numbers and assumptions would require the randomization of 80,000 subjects followed for 5 years. One way to reduce the costs of such a study is to randomize high-risk asymptomatic diabetic patients based on clinical and laboratory criteria as previously proposed, where screening might be expected to be most cost-effective. The problem is that we do not yet know how to select this high-risk asymptomatic group. In the meantime, we should all be cognizant that the entire type 2 diabetic population has to be aggressively managed with prevention strategies, including lifestyle alterations such as weight reduction and exercise, control of atherosclerosis risk factors with medications, and glucose control. Insulin resistance, a major contributor to inflammation, can be treated with drugs. When symptoms such as chest pain or exertional dyspnea emerge, stress imaging for detection of CAD and ischemia are appropriate. We will need to wait for further data before knowing what is appropriate with respect to testing in the totally asymptomatic diabetic population. The essay by Diamond et al. (29) impels us to proceed with future clinical research in this controversial area of cardiovascular medicine.
1. : "Risk stratification in coronary artery disease and special populations (review)". Am J Med 1996; 101: 17S.
2. : "Two alarming recent statistics: the increase in the uninsured and the increased prediction of the number of persons living with diabetes". J Nucl Cardiol 2006; 13: 737.
3. : "National Cholesterol Education Program versus World Health Organization metabolic syndrome in relation to all-cause and cardiovascular mortality in the San Antonio Heart Study". Circulation 2004; 110: 1251.
4. : "Lipids, diabetes, and coronary heart disease: insights from the Framingham Study". Am Heart J 1985; 110: 1100.
5. : "Prevention Conference VI: Diabetes and Cardiovascular Disease: executive summary: conference proceeding for healthcare professionals from a special writing group of the American Heart Association". Circulation 2002; 105: 2231.
6. : "Risk stratification in uncomplicated type 2 diabetes: prospective evaluation of the combined use of coronary artery calcium imaging and selective myocardial perfusion scintigraphy". Eur Heart J 2006; 27: 713.
7. : "Coronary atherosclerosis in diabetes mellitus: a population-based autopsy study". J Am Coll Cardiol 2002; 40: 946.
8. : "Prognostic value of gated myocardial perfusion SPECT (review)". J Nucl Cardiol 2004; 11: 171.
9. : "Impact of diabetes on the risk stratification using stress single-photon emission computed tomography myocardial perfusion imaging in patients with symptoms suggestive of coronary artery disease". Circulation 2002; 105: 32.
10. : "Prognostic value of pharmacological stress echocardiography in diabetic and nondiabetic patients with known or suspected coronary artery disease". J Am Coll Cardiol 2006; 47: 605.
11. : "Yield of stress single-photon emission computed tomography in asymptomatic patients with diabetes". Am Heart J 2004; 147: 890.
12. : "Identifying high-risk asymptomatic diabetic patients who are candidates for screening stress single-photon emission computed tomography imaging". J Am Coll Cardiol 2005; 45: 43.
13. : "Prognostic relevance of symptoms versus objective evidence of coronary artery disease in diabetic patients". Eur Heart J 2004; 25: 543.
14. : "Detection of silent myocardial ischemia in asymptomatic diabetic subjects: the DIAD Study". Diabetes Care 2004; 27: 1954.
15. : "Detection of coronary artery disease in asymptomatic patients with type 2 diabetes mellitus". J Am Coll Cardiol 2006; 47: 65.
16. : "Comparison of the short-term survival benefit associated with revascularization compared with medical therapy in patients with no prior coronary artery disease undergoing stress myocardial perfusion single photon emission computed tomography". Circulation 2003; 107: 2900.
17. : "Prognostic value of coronary artery calcium screening in subjects with and without diabetes". J Am Coll Cardiol 2004; 43: 1663.
18. : "Diabetes and the associated incidence of subclinical atherosclerosis and coronary artery disease: implications for management". Am Heart J 2001; 141: 637.
19. : "Relationship between stress-induced myocardial ischemia and atherosclerosis measured by coronary calcium tomography". J Am Coll Cardiol 2004; 44: 923.
20. : "Severity of coronary artery calcification by electron beam computed tomography predicts silent myocardial ischemia". Circulation 2000; 101: 244.
21. : "Asymptomatic patients with diabetes mellitus should be screened for coronary artery disease". J Nucl Cardiol 2006; 13: 609.
22. : "The potential of myocardial perfusion scintigraphy for risk stratification of asymptomatic patients with type 2 diabetes". J Am Coll Cardiol 2006; 48: 754.
23. : "Should we screen for occult coronary artery disease among asymptomatic patients with diabetes (review)?". J Am Coll Cardiol 2005; 45: 50.
24. : "The role of non-invasive imaging in the risk stratification of asymptomatic diabetic subjects (review)". Eur Heart J 2006; 27: 905.
25. : "Asymptomatic patients with diabetes mellitus should not be screened for coronary artery disease". J Nucl Cardiol 2006; 13: 616.
26. : "Screening asymptomatic diabetic patients for coronary artery disease: why not?". J Am Coll Cardiol 2006; 48: 761.
27. : "Screening for coronary heart disease: cardiology through the oncology looking glass". J Nucl Cardiol 2005; 12: 158.
28. : "Implications of recent clinical trials for the National Cholesterol Education Program Adult Treatment Panel III guidelines (review)". Circulation 2004; 110: 227.
29. : "Screen testing: cardiovascular prevention in asymptomatic diabetic patients". J Am Coll Cardiol 2007; 49: 1915.
30. : The 80/20 Principle . New York, NY: Doubleday1998.
31. : "Screening asymptomatic low-risk individuals for coronary heart disease: issues and controversies". J Nucl Cardiol 2004; 11: 382.
32. : "Prevalence of noncalcified coronary plaques by 64-slice computed tomography in patients with an intermediate risk for significant coronary artery disease". J Am Coll Cardiol 2006; 48: 312.
33. : "Improved survival in asymptomatic diabetic patients with high-risk SPECT imaging treated with coronary artery bypass grafting". Circulation 2005; 112: I311.
34. : "Molecular and metabolic imaging of atherosclerosis (review)". J Nucl Med 2004; 45: 1898.
35. : "Molecular and cellular imaging of atherosclerosis: emerging applications (review)". J Am Coll Cardiol 2006; 47: 1328.
36. : "Detection and treatment of vulnerable plaques and vulnerable patients: novel approaches to prevention of coronary events (review)". Circulation 2006; 114: 2390.
Abbreviations and Acronyms
| CAC | coronary artery calcium |
| CAD | coronary artery disease |
| CT | computed tomography |
| ECG | electrocardiogram |
| LDL | low-density lipoprotein |
| MPI | myocardial perfusion imaging |
| SPECT | single-photon emission computed tomography |
{kind=link}